ORIGINAL ARTICLE
Standard precautions: knowledge and practice of clinical students at the College of Medicine, University of Ibadan
Dimeji Abdulsobur Olawuyi1,2*, Jonas Paul Ibekwe1,2, Oghenemaro Akpooghene Jerry-Ogeme1,2, Aisha Ibrahim1,2, Osaretin Vanessa Ehiorobo1,2, Victoria Oluwamayokun Dada1,2, Emmanuella Chinenye Asogwa1,2, Oluwayomi Victoria Akinkuebi1,2, Ogunleye Moyinoluwa Ayooluwa1,2, Nneka Lilian Amakom1,2 and Chimeziri Ekeledirichukwu Uzondu1,2
1Department of Medicine and Surgery, Faculty of Clinical Sciences, College of Medicine, University of Ibadan, Ibadan, Nigeria; 2Federation of African Medical Students’ Associations Headquarters, Ibadan, Nigeria
Abstract
Background: Hospital-acquired infections are a significant cause of morbidity and mortality in healthcare settings among patients and healthcare workers, including clinical students. The frequent exposure of students during their clinical postings to various sources of infections emphasizes the need for adherence to standard precautions (SP). This study aimed to assess the knowledge and practice of SP among the clinical students of the College of Medicine, University of Ibadan, Nigeria.
Methods: A descriptive cross-sectional study was conducted. Data on sociodemographic, domains of SP knowledge and practice, and source of students’ knowledge were collected via a self-administered online questionnaire. Categorical variables were compared using Chi-square and Z tests, while numerical data were analyzed with Mann–Whitney and Kruskal–Wallis tests. Logistic regression identified predictors of the assessed SP knowledge and practice domains. SPSS v20 was used for data analysis, and P < 0.05 was used as the statistical significance level.
Results: Among 371 clinical students, 55.8% were MBBS students, 78.7% were Christians, and 80.6% were aged 21–25 years. Participants’ overall knowledge score was average, and 131 (36.1%) students scored ≥ 29 (out of 36 points) which was considered an acceptable level of knowledge. The overall practice score was average with a mean practice score of 11.76 (± 2.50) out of 17. Participants’ main sources of knowledge were self-learning and the school curriculum. Logistic regression revealed that participants’ knowledge correlated with gender, year of study, and prior knowledge, while practice correlated with age and department.
Conclusion: The students’ average knowledge and practice and significant reliance on self-learning of SP is alarming. We recommend that universities and medical colleges integrate early and continuous SP education and training into medical curriculum.
Keywords: standard precaution; infection control; knowledge; practice; clinical students
Citation: Int J Infect Control 2026, 22: 23903 – http://dx.doi.org/10.3396/ijic.v22.23903
Copyright: © 2026 Dimeji Abdulsobur Olawuyi et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 22 September 2025; Accepted: 1 November 2025; Published: 29 June 2026
Competing interests and funding: Authors declare no conflict of interest.
No funding was received for this study.
*Mr Dimeji Abdulsobur Olawuyi, Block E, Alexander Brown Hall, University College Hospital, Ibadan, Oyo State, Nigeria, Tel: +234 903 081 6178. Email: lokidimeji@gmail.com
Hospital-acquired infections (HAIs) are a major global public health concern, threatening patient safety and generating extensive financial costs in healthcare settings (1). The prevalence of HAI is higher in low-resource countries compared with developed countries (2). A 2024 systematic review and meta-analysis reveals the prevalence of HAIs in sub-Saharan Africa to be between 6.5 and 19.7% of the patient population, with a mortality of 22.2% (3). Standard precautions (SP), a core component of infection prevention and control, represent the minimum practices to be employed by all healthcare workers while caring for ‘all patients, at all times, in all settings’ (4). The implementation of these precautions aims to reduce nosocomial infections and ensure safe, high-quality healthcare.
However, a significant gap exists between knowledge and practice of hand hygiene among healthcare workers (5). Healthcare providers have been implicated as potential vectors of pathogenic organisms to vulnerable patients (6). Medical students undergoing clinical rotations are a part of the healthcare team, and their interactions with patients during clinical activities may contribute to HAIs (7). They are also at an increased risk of HAIs due to factors including poor “hand hygiene, clothing, and disinfection of medical equipment,” sharing of medical equipment, inhalation of droplets from infected patients, and contact with contaminated surfaces (8, 9). Therefore, undergraduate medical education is a critical phase for acquiring the knowledge and skills necessary for infection prevention and control (10).
Background
HAIs are a significant challenge in healthcare that necessitates integration into the core curriculum of clinical training programs. Providing training sessions to students at the beginning of clinical rotations has been recommended to improve the adherence of clinical students to SP (11). However, infection prevention and control practices are given relatively less focus in medical education (12). A study on perceived barriers to infection prevention and control practices among Nigerian clinical students identified several factors contributing to low compliance, including lack of knowledge, absence of positive role models, gaps between classroom and practical training, inadequate facilities, psychological barriers, and insufficient awareness of SP (13).
Furthermore, studies in Nigerian tertiary hospitals revealed that many students rely on senior colleagues for infection control knowledge due to a lack of formal instruction and inadequate training before clinical rotation (14, 15). Clinical students at Nigerian medical colleges, such as the College of Medicine, University of Ibadan (UI), undertake clinical postings at the University College Hospital (UCH), Ibadan, a tertiary hospital managing high patient volumes, including patients with contagious conditions. Their frequent exposure to nosocomial infections through clinical activities (8, 16) emphasizes the need for targeted interventions.
As a leading tertiary institution, UCH offers a unique setting to evaluate clinical students’ knowledge and practices of SP. This study aims to assess the level of knowledge and adherence to SP among clinical students of the College of Medicine, University of Ibadan and to examine their relationship with sociodemographic characteristics. The outcome of this study will identify critical gaps and inform targeted interventions and curricular improvements across Nigerian medical colleges.
Methodology
Study design, setting, and population
A descriptive cross-sectional study was carried out at the UCH in the Ibadan-North Local Government Area, Ibadan, Oyo state. UCH is a 1,500-bed tertiary care hospital that serves as a major healthcare provider and training center in Nigeria. It was established in 1957 as the first teaching hospital in Nigeria, attached to the UI. UCH houses the College of Medicine, UI, which comprises five faculties: Basic Medical Sciences, Clinical Sciences, Public Health, Dentistry, and Basic Clinical Sciences. These faculties have several departments including Medicine and Surgery, Dentistry, Biomedical Laboratory Science, Physiotherapy, and Nursing. Students in these departments are divided into two groups: pre-clinical and clinical. Clinical training begins in the 3rd year, when students transition to the clinical sections at UCH. Currently, there are 809 clinical students in the College of Medicine, University of Ibadan, comprising those in their 3rd to 6th years of study.
Sampling technique and sample size determination
The minimum sample size for this study was calculated using the formula described by Yamane (1973), n = N / (1 + N(e)2, where n is the sample size; N is the population of the study (809) and e is the margin error of 5% in the calculation. By allowing a 10% contingency, the minimum sample size was determined to be 294.
Data collection
Data were collected through a self-administered anonymous online questionnaire (Supplementary material). Eligible participants were consenting undergraduate clinical students of the College. The participants were recruited into the study by convenience sampling. Clinical students at all study levels from the five departments were contacted through their departmental executive and class representatives. Broadcast messages were also sent to the participants through media platforms like WhatsApp and Telegram. Reminders were sent at the beginning of each week and the last day of data collection. The filling and submission of the anonymized online form indicated consent. The data were collected between September 21 and December 4, 2024.
Research instrument
The study questionnaire was divided into four sections. Following the consent form, the first section collected respondents’ sociodemographic data including gender, religion, age, department (medicine and surgery, dentistry, biomedical laboratory science, physiotherapy, and nursing), prior knowledge of SP, and previous training or orientation on SP.
The second section collected data on respondents’ knowledge of SP, and the third section assessed their practice of SP. Both sections included questions across key domains of SP, including general concepts, hand hygiene, personal protective equipment (PPE), cough etiquette and respiratory hygiene, and sharps disposal and injury. The knowledge section had a total of 36 points, while the practice section had 17 points.
The questionnaire consisted of close-ended questions in multiple-choice or with the options of ‘true’, ‘false’, and ‘I do not know’. The items were adopted from existing literature (17, 18), and the full questionnaire is provided in Additional file 1. Permission for use was obtained from the authors. Correct responses were assigned a score of ‘1’, while incorrect responses/do not know responses were assigned ‘0’.
The fourth section collected data on respondents’ sources of information for each domain of SP, including self-learning, the college curriculum, formal bedside teachings, and bedside practices. The questionnaire was piloted among 45 clinical students to assess feasibility. Face validity, clarity, and comprehension were evaluated with an internal consistency score (Cronbach’s alpha) of 0.74. Participants included 3rd to 6th-year students across the five departments, selected using convenience sampling. The participants were excluded from the main study to prevent duplication and response bias.
Data analysis
Data were imported from Google Forms to Microsoft Office Excel 2019, checked, cleaned, and edited before being exported to SPSS version 20 for analysis. Categorical variables were presented as proportions and percentages, with comparisons made using Chi-square and Z tests. Numerical variables were described using the median, mean, and standard deviation, with comparisons conducted using Mann–Whitney and Kruskal–Wallis statistical tests. Scores for the knowledge domains were summarized using percentiles (not percentages of the total score). The 25th percentile score was 26, the median (50th percentile) was 28, and the 75th percentile was 29 out of a maximum of 36. We used the 75th percentile score of 29 as the cutoff to define sufficient knowledge of SP, i.e. respondents scoring at or above this level performed better than at least 75% of the participants. Similarly, scores for the different practice domains were summarized using percentiles: the 25th percentile score was 10, the 50th percentile was 12, and the 75th percentile was 14 out of a maximum of 17. A score of 14, representing the 75th percentile, was used as the cutoff to define sufficient current practice regarding SP. Logistic regression models were conducted to determine the possible predictors of acceptable knowledge and practice of SP (dependent variables) against the possible independent variables including gender, year at college, age, department (medicine and surgery, dentistry, biomedical laboratory science, physiotherapy, and nursing), prior knowledge of SP, and previous training or orientation on SP. A statistical significance level of 0.05 was used in the analysis.
Results
Sociodemographic characteristics of the respondents
Table 1 summarizes the sociodemographic characteristics and the training exposure of the included participants (N = 371). The majority (35.6%) of the respondents were in the 5th year, and 38.3% of the respondents were females. Most of the respondents were enrolled in the MBBS program (55.8%), followed by Dentistry (14.8%) and Biomedical Laboratory Science (11.9%). A significant percentage of the respondents were Christian (78.7%) and aged 21–25 years (80.6). Of the included participants, 89.8% were familiar with the term ‘standard precautions’, 50% had previous training on SP, and 86.8% were willing to attend future training on SP.
Knowledge of general concepts and hand hygiene
Table 2 shows the responses to knowledge items about the general concepts of SP and hand hygiene by clinical years included. A total of 7.8 and 19.7% of the respondents did not understand the goal of SP and the definition of SP, respectively. The majority of the respondents (85.2%) agreed that all patients are sources of infection, 36.9% recognized all body fluids except sweat as sources of infection, and 99% believed that all health providers are at risk of occupational infection. The overall median score for general concepts was 3.94 ± 0.85 (out of 5), with no significant variation across academic years (P = 0.200).
Regarding hand hygiene, 95.7% of the respondents acknowledged that standard handwashing includes washing both hands and wrists, 25.1% responded that alcohol hand rub substitutes hand washing even if the hands are soiled, 88.4% responded that the use of gloves does not replace handwashing, and 82.5% correctly stated the minimum duration of hand washing. The overall median score for hand hygiene was 8.30 ± 0.93 (out of 10 points), with no significant variation across academic years (P = 0.197).
Knowledge of PPE and cough etiquette and respiratory hygiene
Table 3 presents responses to knowledge items about the appropriate use of PPE. A majority of respondents (62.3%) believed that the use of PPE eliminates the risk of acquiring occupational infections, while 12.1% stated that PPE should only be used when there is contact with blood. Additionally, 91.6% disagreed that gloves and masks can be reused after proper cleaning. Furthermore, 72.2% acknowledged that gloves should be changed between different procedures on the same patient, and 49.6% believed that masks made of cotton or gauze are the most protective. The overall median score for this domain was 6.39 ± 145 (out of 9 points), with significantly higher scores among those in the 6th year (P = < 0.001) (Figure 1).
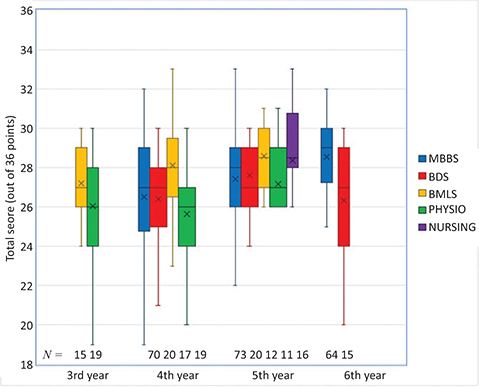
Figure 1. Total knowledge scores of participants about SP in relation to department and year of study. SP: standard precautions.
Table 3 also presents responses to knowledge items on cough etiquette and respiratory hygiene. Nearly all respondents (96.8%) acknowledged that it is appropriate to cough or sneeze into a disposable tissue and perform hand hygiene, while 95.1% agreed that coughing into an elbow is appropriate if a tissue is unavailable. Additionally, 93% stated that maintaining a distance of 1 meter from others when coughing is appropriate, and 15.4% believed that it is acceptable to wipe hands on the inside of ward coats after coughing or sneezing. The overall median score for this domain was 3.70 ± 0.58 (out of 4 points), with no significant variation across academic years (P = 0.476).
Knowledge of sharps disposal and sharps injuries
Table 4 presents responses to knowledge items on appropriate sharps disposal and sharp injuries management. Surprisingly, 79.2% of respondents stated that used needles should be recapped after use to prevent injuries, while 24.3% agreed that used needles should be bent after use. In addition, 89.5% acknowledged sharps injuries should be managed by reporting the incident, and 81.1% believed that needle-stick injuries are most commonly encountered in general practice. The overall median score for this domain was 4.96 ± 1.21 (out of eight points), with no significant variation across academic years (P = 0.289).
The total score for the respondents’ knowledge of the domains of SP practices was 27.29 ± 2.97 (out of 36).
Acceptable level of knowledge and its correlates
The cutoff for sufficient knowledgeable of SP was set at the 75th percentile (≥ 29 out of a total of 36 points). Overall, 131 (36.1%) students achieved scores ≥ 29, 8/34 (23.53%) in 3rd year, 36/126 (28.57%) in 4th year, 47/132 (36.61%) in 5th year, and 43/79 (54.43%) in 6th year. By department, 83/207 (40.10%) MBBS students, 15/55 (27.27%) dentistry students, 18/44 (40.91) BMLS students, 10/49 (20.41%) physiotherapy students and 8/16 (50.00%) nursing students scored ≥ 29.
Table 5 presents the results of binary regression analysis. Knowledge scores were significantly correlated with gender, year of study, and prior knowledge of SPs, while age, department, previous training or orientation on SPs, and practice scores were not significantly associated with knowledge scores.
Sources of students’ knowledge
Figure 2 depicts medical students’ major sources of information across the different domains of SP. Except for the general concept domains, the current curriculum was not cited as the main source of knowledge, particularly for cough etiquette and respiratory hygiene and sharps management. Most students reported self-learning as their main source of information on SP.
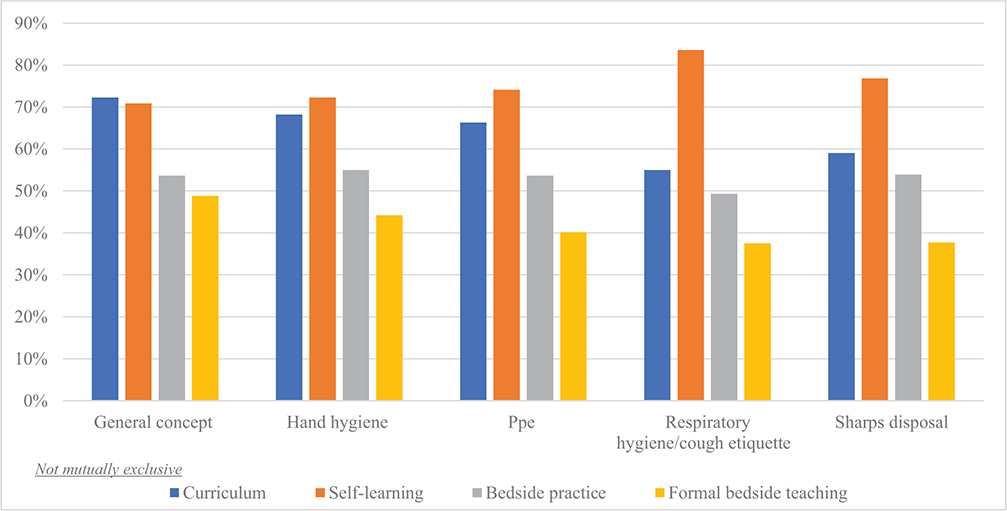
Figure 2. The main sources for information about the different domains of SP among the participants. PPE: personal protective equipment.
Table 6 presents the practice of SP among clinical students by academic year. For the domain of hand hygiene, only 45% of respondents followed all eight steps of handwashing, while 74.12% reported washing their hands even if they did not touch patients. The overall median score for this domain was 1.91 ± 0.97 (out of three points), with no significant variation across academic years (P = 0.920).
For the domain of cough etiquette and respiratory hygiene, 85.98% of the surveyed respondents reported coughing or sneezing into their elbows if tissues are not available and only 15.36% receive annual influenza vaccination. The overall median score for this domain was 2.59 ± 0.93 (out of four points), with significantly higher scores among those in 3rd year (P = < 0.032).
For the domain of PPE, 78.17% of respondents reported using appropriate PPE for potential splashes and spills of body fluids; 33.42% reported wearing jewelry or keeping personal belongings on while wearing PPE. Notably, 44.74% reported wearing coats or scrubs outside of the hospital. The overall median score for this domain was 3.43 ± 1.31 (out of five points), with significantly higher scores among those in 3rd year (P = < 0.030).
For the domain of sharps disposal and injuries, 79.78% of respondents reported recapping needles and 97.3% responded that they do follow proper techniques for handling and disposing of sharps. The overall median score for this domain was 3.83 ± 0.70 (out of five points), with significantly higher scores among those in 5th year (P = < 0.001). The total score for the respondents’ reported SP practices was 11.76 ± 2.50 (out of 17).
Table 7 presents the results of the binary regression analysis. Practice scores were significantly correlated with the age and department (medicine and nursing), while gender, year at the college, department (dentistry, medical laboratory science, and physiotherapy), prior knowledge of SP, previous training or orientation on SP, and knowledge scores were not significantly associated with practice scores.
Discussion
In this study, we assessed the knowledge and practice of SP among clinical students at the College of Medicine, University of Ibadan, Nigeria. Based on the 75th percentile cutoff (29 out of 36 points), only 36.1% of students demonstrated sufficient knowledge about SP, despite the majority (89.8%) having heard of the term and half (50.1%) having received prior training. This discrepancy may indicate exposure without structured learning. Moreover, prior training may have been infrequent, or limited to one–off sessions without reinforcement or clinical integration, thereby affecting knowledge retention.
These findings are supported by studies among Nigerian healthcare workers in Enugu State which reported only 27.3% having good knowledge level (19), despite using a cutoff of 50%, as well as studies in Edo State (10.6%) (20), Cross River State, (58%) (21), and Uganda (57.2%) (22). However, a prior study among clinical students at the College of Medicine, University of Ibadan, showed 91.6% of the participants had good knowledge (13). This high value may be attributed to the use of an interviewer-administered structured questionnaire, which may have influenced respondents’ answers.
Knowledge of SP among clinical students and HCWs can significantly impact healthcare practice, potentially increasing morbidity and mortality among patients while also contributing to antimicrobial resistance if not properly taught and implemented (19). Therefore, greater emphasis on SP is necessary in both academic and healthcare settings through continuous professional development training using a robust curriculum. The need for such a comprehensive curriculum is evident from the finding that most participants acquired knowledge of four out of five SP domains primarily through self-learning. This aligns with findings among HCWs in Benue (23) and Edo states (20) in Nigeria, as well as among clinical students in Uganda (24). In contrast, a study at King Saud bin Abdulaziz University, Saudi Arabia (25), reported that formal curricular teaching was the primary source of SP knowledge.
Despite the average overall knowledge level, most participants correctly answered questions on general SP concepts, with a mean score of 78.8%. However, participants lacked proper knowledge of which body fluids should be considered potentially infectious, as 63.1% incorrectly believed that all body fluids except sweat are non-infectious. According to the World Health Organization, several body fluids including blood, breast milk, semen, vaginal secretions, serous fluids, cerebrospinal fluid, and amniotic fluid should be considered potentially infectious, because they can easily harbor high concentrations of viral particles, even in asymptomatic carriers (26). In contrast, participants demonstrated good knowledge of hand hygiene, with an overall mean score of 83%. More than 70% of participants provided the correct answers to each knowledge statement, except for hand decontamination (28.3%). This finding is consistent with reports by Nwoga et al. (27), where over 90% of participants provided the correct answers to each knowledge statement.
Regarding the use of PPE, cough etiquette/respiratory hygiene, and sharps disposal/sharp injuries, the overall mean scores were 71, 92.5, and 62%, respectively. Most questions were answered correctly, particularly those related to cough etiquette/respiratory hygiene, where at least 84.6% of participants provided the correct responses. Similarly, an assessment of SP among HCWs in a tertiary health facility in Enugu State (27) yielded comparable results, as did a prior study among clinical nursing and medical students at the UCH, Ibadan (13). The majority (79.2%) of our study participants incorrectly believed that needles should be recapped after use, compared to 41.8% reported by Amali et al. (23), and 61.7% were unaware that sharps should be shredded before final disposal.
Based on the percentile cutoff, clinical students at the College reported an average level of SP practice (12 out of 17 points), with an overall mean score of 69.2%. Notably, only 45.01% of students followed the eight steps of handwashing, in contrast to a study at Bayero University, Kano State, where 62.8% adhered to proper handwashing techniques during clinical postings (28). This difference may reflect variations in students’ attitudes and perceived importance of handwashing, as well as time pressure during rotations, fatigue or stress in busy clinical environments. In regard to vaccination, only 15.36% of our respondents reported receiving annual influenza vaccination. In comparison, a study involving medical students from seven institutions in southeastern Nigeria found that 40.5% had received the necessary vaccines (29). Despite the significance of influenza as a cause of respiratory illness in Nigeria (30), the low vaccination rate could be attributed to factors such as a lack of trust in government health initiatives, poor perception of vaccine safety and efficacy, a perceived lack of vulnerability to the virus, and insufficient information about vaccine availability (31). These barriers have been reported even among the educated populations in Nigeria (31, 32).
Additionally, 79.78% of participants reported recapping needles. Similar findings were reported among HCWs in Enugu State (69.5%) (27). Furthermore, 84.64% of respondents reported not reusing sharps on the same patient, while 92.45% disposed of sharps in appropriately labelled containers. Overall, there is a need to improve knowledge of appropriate sharps disposal and injury prevention among students and HCWs.
Logistic regression analysis showed that SP knowledge among clinical students was significantly associated with gender, year of study, and prior knowledge of SP, in contrast to a study by Emilia et al. who reported only age and profession/department as significant factors (22). In our study, female students demonstrated better SP knowledge, contrary to findings in other studies where male students exhibited higher knowledge levels (33). Surprisingly, only age and department (medicine and nursing) were significant predictors of SP practice among clinical students. In comparison, Emilia et al. found an association only between profession/department and SP practice (22). These differences may be due to variations in sample sizes, sampling methods, and participant composition across studies. Although no direct association was found between SP knowledge and practice scores in this study, improving SP knowledge among students and HCWs, remains important to reducing the spread of infections in healthcare settings (19, 34, 35).
Based on the findings of this study, health institutions and organizations should prioritize structured training of students and staff on SP to improve the quality and outcomes of patient care. As key centers for healthcare education, colleges of medicine should establish clear policies and implement mandatory, continuous regular reinforcement through clinical teaching, and routine meetings may help address practical challenges, strengthen positive attitudes, and promote sustained adherence to SP guidelines.
This study has several limitations. Its cross-sectional design limits, the ability to establish causal relationships, and the use of convenience sampling may affect the generalizability of the findings. In addition, reliance on self-reported data may introduce recall and social desirability bias. Direct observation of participants’ skills and adherence to SP was not feasible due to variations in clinical rotations across departments. Nonetheless, the relatively large sample size and inclusion of participants from multiple departments within the College enhance the representativeness and overall relevance of the findings.
Conclusion
The overall knowledge and practice of SP among students of the College of Medicine, University of Ibadan, were moderate across several domains. The finding that most students relied on self-learning as their primary source of SP knowledge highlights a gap in the formal curriculum. We recommend that universities and colleges integrate structured SP training into medical education from the early years, prior to the commencement of clinical rotations. In addition, continuous, hands-on training in infection prevention and control should be provided to reinforce these practices. Future research should include broader, multi-institutional samples and incorporate observational methods to assess practice more objectively.
Ethics approval and consent to participate
This study was conducted in full compliance with the principles outlined in the Declaration of Helsinki. All procedures involving human participants were reviewed and approved by the ethical committee of the University of Ibadan/University College Hospital (UI/UCH) with the assigned number UI/EC/24/0519. Also, the online form contained the objective of the study, and a question seeking informed consent was also added. Only the responses of respondents who agreed to the informed consent were included.
Authors’ contributions
DAO conceptualized the research; DAO, JPI, OAJ, AI, OVE, VOD, ECA, OVA, OMA, and CEU designed the study; DAO, JPI, OAJ, AI, OVE, VOD, ECA, OVA, OMA, NLA, and CEU collected data; DAO analyzed and visualized data; OAJ, AI, OVA, and NLA drafted the introduction, DAO drafted the methodology and results; JPI, ECA, and CEU drafted the discussion; OMA drafted the conclusion; DAO, JPI, OAJ, AI, OVE, VOD, ECA, OVA, OMA, NLA, and CEU drafted and reviewed the final manuscript. All authors approved the manuscript for submission and agreed to be accountable for all aspects of the work.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgements
We express our immense gratitude to Prof. Adeola Fowotade for supervising this research and reviewing the manuscript. We appreciate David Magbadelo for his assistance with data analysis. Also, we appreciate Babatunde Dauda, Ridwan Agboola, Mubarak Alimi, Damilare Oluwo, Victor Adediran, Theophilus Akintoye, Favour Adegbile, Ibitoye Oluwatobiloba, and all students of the College of Medicine, University of Ibadan, for their assistance and cooperation during data collection.
Supplementary material - Research questionnaire
This file contains the questionnaire used for data collection in this study. The questionnaire assesses participants’ knowledge and practice of standard precautions and infection control. It includes sections on socio-demographic characteristics, knowledge of standard precautions and infection control, practice of standard precautions and infection control, and source of participants’ knowledge of standard precautions and infection control. The questionnaire was adopted from the existing literature.
References
| 1. | Orlando S, Cicala M, De Santo C, Mosconi C, Ciccacci F, Guarente L, et al. The financial burden of healthcare-associated infections: a propensity score analysis in an Italian healthcare setting. Infect Prev Pract 2024; 7(1): 100406. doi: 10.1016/j.infpip.2024.100406 |
| 2. | Gozel MG, Hekimoglu CH, Gozel EY, Batir E, McLaws ML, Mese EA. National Infection Control Program in Turkey: the healthcare-associated infection rate experiences over 10 years. Am J Infect Control 2021; 49(7): 885–92. doi: 10.1016/j.ajic.2020.12.013 |
| 3. | Melariri H, Freercks R, van der Merwe E, Ten Ham-Baloyi EW, Oyedele O, Murphy RA, et al. The burden of hospital-acquired infections (HAI) in sub-Saharan Africa: a systematic review and meta-analysis. EClinicalMedicine 2024; 71: 102571. doi: 10.1016/j.eclinm.2024.102571 |
| 4. | World Health Organization. Standard precautions for the prevention and control of infections: aide-memoire. Geneva: WHO; 2022. Available from: https://www.who.int/publications/i/item/WHO-UHL-IHS-IPC-2022.1 [cited 11 February 2024]. |
| 5. | Ahmed J, Malik F, Memon ZA, Arif TB, Ali A, Nasim S, et al. Compliance and knowledge of healthcare workers regarding hand hygiene and use of disinfectants: a study based in Karachi. Cureus 2020; 12(2): e7036. doi: 10.7759/cureus.7036 |
| 6. | Oyapero A, Oyapero O. An assessment of hand hygiene perception and practices among undergraduate nursing students in Lagos State: a pilot study. J Educ Health Promot 2018; 7: 150. doi: 10.4103/jehp.jehp_56_17 |
| 7. | Shyaka M, Nzisabira J, Mfura H, Tuli S, Glynn L. Medical healthcare students’ knowledge, attitude, and practices regarding hand hygiene and its relation to patient safety – a global scoping review. Adv Med Educ Pract 2024; 15: 1041–55. doi: 10.2147/amep.s283642 |
| 8. | Awab A, Sittana S. Knowledge, awareness, and attitude regarding infection prevention and control among medical students: a call for educational intervention. Adv Med Educ Pract 2016; 7: 505–10. doi: 10.2147/amep.s109830 |
| 9. | Ishwari SP, Vivek G, Purushottam A. Knowledge, attitude and practice of nursing students on hospital-acquired infections in Western Region of Nepal. J Coll Med Sci-Nepal 2016; 10: 3126. |
| 10. | Okonkwo PI, Okafor KC, Garbal JH, Kwaghal BS, Boluwatito B. Hospital-acquired infections (HAIs) prevention practices among medical students in a teaching hospital in Jos, Plateau State, Nigeria. Eur J Med Health Sci 2024; 6(2): 14–20. doi: 10.24018/ejmed.2024.6.2.2020 |
| 11. | Nath S, Kumar N, Kumar R. Comparative study on knowledge of hand hygiene among medical students, resident doctors, and nurses at tertiary health institution of Uttar Pradesh. Asian J Pharm Clin Res 2022; 15(9): 162–6. doi: 10.22159/ajpcr.2022.v15i9.45097 |
| 12. | Tingelhoff PD, Hufert F, Kiessling C, Otto B. Infection prevention in medical education – results of a descriptive cross-sectional study in Germany. GMS Z Med Ausbild 2024; 41(1): Doc4. doi: 10.3205/zma001659 |
| 13. | Akinwaare MO, Bello KO, Ani O. Perceived barriers, knowledge and reported practices of infection prevention and control among clinical nursing and medical students of a Nigerian University. Int J Infect Control 2020; 16(4): 20. doi: 10.3396/ijic.v16i4.025.20 |
| 14. | Muoneke VU, Okechukwu AA, Egwuonwu OA. Knowledge of standard precautions among medical students in a tertiary hospital in Nigeria. Niger J Clin Pract 2018; 21(2): 211–16. |
| 15. | Priyanka D, Agarwal S, Mohan R. Barriers to infection control practice among medical students. Asian Pac J Public Health 2020; 32(6): 384–90. |
| 16. | Chauhan S. Medical student exposure to nosocomial infections: an overlooked risk factor in infection control. Indian J Med Microbiol 2017; 35(1): 76–81. |
| 17. | Amin TT, Al Noaim KI, Bu Saad MA, Al Malhm TA, Al Mulhim AA, Al Awas MA. Standard precautions and infection control, medical students’ knowledge and behavior at a Saudi university: the need for change. Glob J Health Sci 2013; 5(4): 114–25. doi: 10.5539/gjhs.v5n4p114 |
| 18. | Aarthy A, Chellaiyan VGD, Vishalini A. Assessment of infection prevention and control practices among medical students of a medical college in Chengalpattu District, Tamil Nadu. J Commun Dis 2022; 54(2): 12–18. doi: 10.24321/0019.5138.202265 |
| 19. | Ochie CN, Aniwada EC, Uchegbu EK, Asogwa TC, Onwasoigwe CN. Infection prevention and control: knowledge, determinants and compliance among primary healthcare workers in Enugu metropolis, south-east Nigeria. Infect Prev Pract 2022; 4(2): 100214. doi: 10.1016/j.infpip.2022.100214 |
| 20. | Osagiede E, Utomi S, Egbuta O, Osagiede E, Airefetalor I, Abah S. Knowledge and practice of standard precautions for infection prevention and control among health care workers in public primary and secondary health facilities in Edo State: a reflection of the neglect of first and second levels of care in infection prevention. J BioMed Res Clin Pract 2020; 3(4): 435–43. doi: 10.46912/jbrcp.199 |
| 21. | Oluwafemi OF, Jonathan OA, Nsa EB, Michael AA, Msoo AJ. Knowledge and practice of infection prevention and control among healthcare workers in secondary healthcare facilities in Southern Cross River State Nigeria. Niger J Med 2024; 33(1): 80–8. doi: 10.4103/njm.njm_56_23 |
| 22. | Emilia AE, Aheebwa A, Obiezu EJ, Jennifer E, Abdulmuminu I, Narayana G, et al. Knowledge and predictors of implementation of standard precautions for infection prevention and control among health care practitioners. Afr J Infect 2024; 18(2 Suppl): 22–33. doi: 10.21010/Ajidv18i2S |
| 23. | Amali OO, Van Wyk RH. Infection prevention knowledge and practices among healthcare workers at a health facility in Makurdi, Benue State, Nigeria. J Public Health Afr 2023; 14(11): 9. doi: 10.4081/jphia.2023.2599 |
| 24. | Nalunkuma R, Nkalubo J, Abila DB. Knowledge on infection prevention and control and associated factors among undergraduate health professional students at Makerere University College of Health Sciences, Uganda. PLoS One 2021; 16(8): e0255984. doi: 10.1371/journal.pone.0255984 |
| 25. | Khubrani A, Albesher M, Alkahtani A, Alamri F, Alshamrani M, Masuadi E. Knowledge and information sources on standard precautions and infection control of health sciences students at King Saud bin Abdulaziz University for Health Sciences, Saudi Arabia, Riyadh. J Infect Public Health 2017; 11(4): 546–9. doi: 10.1016/j.jiph.2017.10.013 |
| 26. | World Health Organization. HIV and AIDS. 2024. Available from: https://www.who.int/news-room/fact-sheets/detail/hiv-aids [cited 30 April 2024]. |
| 27. | Nwoga H, Ajuba M, Chime O. Standard precautions among HealthCare workers in a Tertiary Health Facility in Enugu Metropolis, South-East Nigeria. Rwanda J Med Health Sci. 2021; 4(3): 366–78. doi: 10.4314/rjmhs.v4i3.6 |
| 28. | Mohammed A, Aliyu I. Hand-washing practices and techniques among clinical students of Bayero University Kano, Nigeria. Sudan Med Monitor 2015; 10(2): 51. doi: 10.4103/1858-5000.160942 |
| 29. | Ekwebene OC, Edeh CG, Azubuike PC, Phyllis NC, Obi CA, Abazu SD, et al. Knowledge, Attitude, and practices regarding infection control measures among clinical medical students in South Eastern Nigeria. Am J Med Clin Sci 2022; 7(1): 1–8. doi: 10.33425/2832-4226/22001 |
| 30. | Akano A, Sadauki AH, Adelabu AM, Malgwi A, Fagbola M, Ogunbode O, et al. Epidemiology of influenza in Nigeria: a secondary analysis of the sentinel surveillance data in Nigeria from 2010–2020. J Infect Public Health. 2024; 17(3): 495–502. doi: 10.1016/j.jiph.2023.12.021 |
| 31. | Ibekwe JL, Femi-Lawal VO, Thomas JA, Okei FU, Ojile MO, Akingbulugbe OO. Nigerians’ attitudes and perceptions towards vaccine acceptance during and after the COVID-19 pandemic. J Med Surg Public Health 2024; 2: 100066. doi: 10.1016/j.glmedi.2024.100066 |
| 32. | Olawuyi DA, Esanju DO, Olowolayemo SA, Asogwa CS, Salako OO, Kolajo AE, et al. Immunization of children in Africa: strides and challenges. Niger J Med 2023; 32(3): 229–34. doi: 10.4103/njm.njm_42_23 |
| 33. | Alshammari SA, Alrasheed SS, Alruhaimi WA, Albnyan AI, Alruhaimi B, Hajj M. Knowledge, attitude, and practice of standard infection control precautions among medical students at King Khalid University Hospital. Cureus 2024; 16(6): e62768. doi: 10.7759/cureus.62768 |
| 34. | Ogoina D, Pondei K, Adetunji B, Chima G, Isichei C, Gidado S. Knowledge, attitude and practice of standard precautions of infection control by hospital workers in two tertiary hospitals in Nigeria. J Infect Prev 2015; 16(1): 16–22. doi: 10.1177/1757177414558957 |
| 35. | Abalkhail A, Imam MHA, Elmosaad YM, Jaber MF, Hosis KA, Alhumaydhi FA, et al. Knowledge, attitude and practice of standard infection control precautions among health-care workers in a University Hospital in Qassim, Saudi Arabia: a cross-sectional survey. Int J Environ Res Public Health 2021; 18(22): 11831. doi: 10.3390/ijerph182211831 |