ORIGINAL ARTICLE
Fungal reservoirs in the hospital environment: prevalence and factors associated with Aspergillus contamination of bed rails in a tertiary hospital in Nigeria
Olufunmilola Makanjuola1,2*, Gloria Igbor3 and Florence Bamigbola2,3
1Department of Medical Microbiology and Parasitology, College of Medicine, University of Ibadan, Ibadan, Nigeria; 2Department of Medical Microbiology and Parasitology, University College Hospital, Ibadan, Nigeria; 3Department of Biomedical Laboratory Science, College of Medicine, University of Ibadan, Ibadan, Nigeria
Abstract
Background: Aspergillus species are common environmental fungi known to cause Aspergillosis, often presenting as an invasive infection in individuals with a compromised immune system. It is transmitted by the inhalation of Aspergillus spores and contributes to healthcare associated infections in hospitalised patients. Since these patients spend most of the day in their hospital beds, the presence of Aspergillus spores in such settings puts the patient at risk of inhaling aerosolised spores leading to infections.
Objective: To determine the prevalence, distribution, and factors associated with Aspergillus contamination of hospital bed rails.
Design: This laboratory-based cross-sectional study was carried out at the University College Hospital, Ibadan, Southwest Nigeria, between May and June 2023. In all, 100 beds which were occupied by patients in 13 wards were included in this study. The left and right rails of beds were swabbed and processed for the detection of Aspergillus species using fungal culture and microscopy. A checklist was used to assess selected infection prevention and control measures in the wards.
Results: The total number of bedrails with Aspergillus isolated across all the wards where samples were taken was 56 (28.0%). Aspergillus niger was the most prevalent specie (64.2%) followed by Aspergillus flavus (30.4%), then Aspergillus fumigatus (5.4%). The prevalence of Aspergillus contamination was related to the level of sanitation and proximity to construction activity.
Conclusion: To reduce the risk of Aspergillus infections in hospitalised patients, adequate infection prevention and control measures including thorough cleaning and disinfection should be strictly adhered to.
Keywords: Aspergillus flavus; Aspergillosis; invasive fungal infections; healthcare associated infections; infection control
Citation: Int J Infect Control 2026, 22: 23864 – http://dx.doi.org/10.3396/ijic.v22.23864
Copyright: © 2026 Olufunmilola Makanjuola et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 3 June 2025; Accepted: 8 November 2025; Published: 28 April 2026
Competing interests and funding: All authors declare that there is no conflict of interest with respect to this article. This is a self-funded study, we did not receive any funding.
*Olufunmilola Makanjuola, Department of Medical Microbiology and Parasitology, College of Medicine, University of Ibadan, P.M.B 5017 G.P.O Ibadan, Oyo State, Nigeria. Email: funmimakanjuola@yahoo.com
Nosocomial or healthcare associated infections (HAIs) which include bacterial, viral, and fungal infections may occur in patients receiving medical care. These infections are seen in both developed and developing countries, though global estimates report higher burden in developing nations (1). According to the World Health Organization (WHO), approximately 15.0% of all hospital patients suffer from these infections (2). The route of HAI transmission includes airborne, droplet, contact, common vehicles, medical devices, and instrumentation (3). As these infections occur during hospital stay, they cause prolonged hospitalisation, disability, and increased economic burden (1). The increasing number of HAIs, especially opportunistic fungal infections, has received significant attention in recent decades as they constitute a great threat to patient health and safety (4, 5).
Aspergillus species are spore-forming fungi widely distributed in soil, water, and decomposing vegetation (6). In the healthcare settings, Aspergillus species can also be isolated from various surfaces and materials including unfiltered air, dirt from suspended ceilings, dust released from hospital renovation, and construction works which settle on surfaces, healthcare equipment, and devices such as ventilation devices, catheters, and implants (7). Aspergillus species can cause or contribute to the development of several diseases including sinusitis, allergic bronchopulmonary disease, mycotic keratitis, otomycosis and in severe cases, invasive aspergillosis, In addition, the fungus may also spread into the bloodstream and disseminate to various organs (8). Aspergillus infections develop from inhalation of the fungal spores (conidia) and are often implicated in HAIs particularly in patients with compromised immune systems (9).
Large construction activities, humidity, temperature, and location of hospital are some of the factors that affect their environmental density (10). High density of Aspergillus spores in the clinical environment is a high-risk situation for immunocompromised patients such as Advanced human immunodeficiency virus disease (AHD) patients, patients with malignancies, and elderly individuals (11, 12). Although Aspergillus fumigatus and Aspergillus flavus are usually the most commonly isolated species, at least 30 species including A. terreus, A. niger, A. versicolor, A. nidulans, and A. ustus have been implicated in human disease (13). It is therefore important to accurately identify the species causing infection to ensure adequate and appropriate treatment (14). Many research articles have documented Aspergillus air contamination in health facilities, however, few have investigated contamination of surfaces in such environments.
The aim of this research was to determine the prevalence, distribution, and factors associated with Aspergillus species on bed rails of wards at the University College Hospital as a means of assessing the risk of fungal HAIs in hospitalised patients.
Methods
This was a laboratory-based cross-sectional study carried out in the University College Hospital, a 1,000-bed a public tertiary hospital located in Oyo state, a region in the South-Western part of Nigeria. A total of 13 wards were purposively selected for the study, and ward type with assigned numbers were used to de-identify the wards. The samples were collected for a period of 1 month from mid-May to mid-June 2023, and the beds sampled were those occupied by patients at the time of data collection. The left and right rails of the beds were swabbed with the aid of a sterile swab stick moistened in normal saline. The swab sticks were labelled with a unique laboratory number, name of the ward, date, and time of collection. Collected samples were put into a Ziploc bag, sealed securely, and transported to the Medical Microbiology Laboratory, University College Hospital, Ibadan, within 1 h of collection. For each ward, a checklist was used to assess selected environmental infection prevention and control measures. The swabs from the bed rails were processed for fungal isolation following standard microbiological procedures (15). Each swab was streaked on Sabouraud Dextrose Agar plate supplemented with chloramphenicol to further inhibit bacterial growth. The plates were incubated for 2–5 days at room temperature and observed daily for growth. Once colonies were visible, their morphology, colonial form, and surface and reverse colour and other macroscopic characteristics were assessed. Microscopic examination was performed using lactophenol cotton blue wet mount to examine the form and arrangement of spores and spore-bearing structures in order to identify the Aspergillus species.
Data entry and analysis were done using the Statistical Package for the Social Sciences (SPSS) version 25 software package. Data were summarised using frequencies, percentages, means among others, and presented as tables and charts. Categorical data including prevalence of Aspergillus species, distribution of Aspergillus species across each ward, and factors associated with contamination were summarised as frequencies and proportion and presented as tables and charts. Quantitative data were summarised as range and mean values. A score of 0 (poor) or 1 (good) was assigned to the observation for each of the six parameters on the checklist. The total score out of a maximum obtainable score of 6 was converted to a percentage.
Results
A total of 100 beds were included in this study, and overall, 200 samples were obtained from swabbing the left and right rails of the various beds. The occurrence of industrial action by health workers during data collection resulted in two sets of research data. Batch 1 data were collected during the regular work period while Batch 2 data were those collected during the industrial action.
As shown in Table 1, surgical ward 1 (15.0%) and medical ward 2 (15.0%) had the highest numbers of bed rails swabbed due to the higher number of occupied beds at the time of sampling while medical ward 3 had the least number of bed rails swabbed (2.0%). Table 2 shows the total number of bed rails swabbed per ward, the corresponding number with Aspergillus growth, and the prevalence of Aspergillus contamination. The overall prevalence of Aspergillus on bed rails was 28.0%. The prevalence of Aspergillus contaminated bed rails per ward was higher in wards where samples were taken during the industrial strike action as compared to those taken before the industrial strike action with surgical ward 3 having the highest prevalence of 55.0%, and medical ward 6 with the least prevalence of 6.3%. Table 3 shows the percentages of the various Aspergillus species which were isolated in this study. Three species of Aspergillus were identified: Aspergillus niger (64.2%) was the most isolated specie followed by Aspergillus flavus (30.4%) then Aspergillus fumigatus (5.4%).
| Organisms isolated | Frequency (n) | Percentage (%) |
| Aspergillus flavus | 17 | 30.4 |
| Aspergillus fumigatus | 3 | 5.4 |
| Aspergillus niger | 36 | 64.2 |
| TOTAL | 56 | 100.0 |
Figure 1 shows the rust and dust characteristics of the various bed rails which were swabbed. A total of 30 bed rails were rusty, 58 were dusty/dirty, and four were both. Aspergillus contamination rate was higher on bed rails with dirt than the rusted ones. About 33% of dusty bed rails yielded Aspergillus, while this was only 7% for rusted rails. Half of the bed rails that were both dusty and rusted had Aspergillus contamination. Of the dusty bed rails 7 had A. flavus contamination, 1 had A. fumigatus and 13 had A. niger. Only 2 of the rusted rails had A. flavus, while none had A. fumigatus nor A. niger.
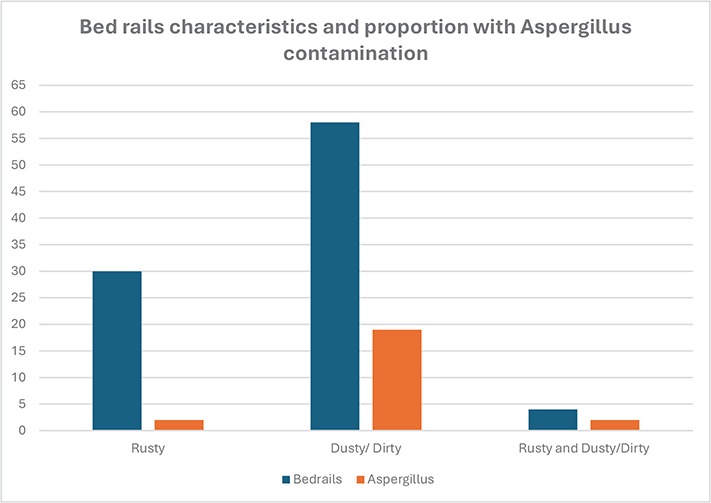
Figure 1. Bed rails characteristics and Aspergillus contamination.
Assessment of the various wards for infection control processes using selected components of the built environment is shown in Table 4. Most of the suboptimal characteristics were observed on the wards where sample collection was done during the industrial action. Overall, eight of the 13 wards had obvious litter such as cotton wool, syringe packs, and biscuit wraps on the floor surface. While 10 wards had adequate numbers of waste bins 3 wards had overfilled waste bins. Ten wards had at least two functional handwash stations, which was the adequate number for such wards. All the wards were well ventilated and no visible moulds were seen on the wall or ceiling surfaces.
Table 5 shows the scores obtained by each ward as computed from the built environment assessment. All wards sampled during routine work period had high scores of 83.3% and 100.0% (mean score 91.7%) while those sampled during the industrial action had scores ranging from 33.3% to 100.0% (mean score 66.7%). There was a slightly higher but insignificant difference between the average scores for surgical wards (76.2%) compared to medical wards (72.2%).
Discussion
The incidence of fungal infections has continued to surge globally, mainly due to the increasing population of patients who are immunocompromised (16). In both developing and developed countries, fungal infections are a major health challenge as these immunocompromised patients are prone to life-threatening systemic fungal infections particularly within the hospital environment (17, 18). In all, 56 Aspergillus species were isolated from a total of 200 samples giving a 28.0% prevalence of Aspergillus species on bed rails. This high prevalence is worrisome as bed rails are considered high-touch surfaces in the hospital environment, and such a level of contamination poses a significant risk for healthcare-associated transmission of Aspergillus to vulnerable patients.
Our study isolated three Aspergillus species, A. niger, A. flavus, and A. fumigatus with A. niger predominating. Data from available studies show a high diversity in the prevalence and distribution of the various Aspergillus species in the hospital environment (19–21). Several reports align with our finding, identifying A. niger as the predominant Aspergillus spp which is widely distributed in the environment. Jangi et al. in a Malaysian University hospital identified A. niger as the most common of 102 fungal isolates from the environmental samples such as the hospital interior spaces and equipment, bedsheets, air, walls, and air conditioning (19).
Although A. niger is less frequently associated with invasive infections, exposed patients are at risk of localised infections such as otomycosis and allergic manifestations particularly Allergic Bronchopulmonary Aspergillosis (ABPA) (22). Karalti et al. monitored the Aspergillus species in six different hospitals in Istanbul for 1 year and reported a predominance of A. niger (11). However, they reported a remarkably greater diversity of Aspergillus species including A. candidus, A. cervinus, A. flavipes, A. flavus, A. fumigatus, A. nidulans, A. niger, A. niveus, A. ochraceus, A. reptans, A. restrictus, A. ustus, and A. versicolor.
In contrast to our observation of A. flavus accounting for about one third of our isolates and the second most common species, Diba et al. reported A. flavus as the predominant species in four educational hospitals in Iran during an 18-month period, accounting for 55.0% of clinical and environmental isolates (14). A. flavus is known to cause allergic and invasive disease in both immunocompetent and immunocompromised individuals, ranking second to A. fumigatus in prevalence. The observation of Diba et al. is however not unusual as their study was conducted in a region where A. flavus is the predominant etiological agent for Aspergillus infection (23).
We observed that a higher proportion of dusty bed rails yielded Aspergillus compared to the overall prevalence of Aspergillus on the bed rails (32.8% vs. 28.0%), while an even higher proportion of 50.0% was seen in beds that were both dusty and rusted. This finding is not surprising as dust particles can trap Aspergillus spores and settle on various surfaces (24). Our observations reinforce the importance of adequate cleaning in curbing microbial contamination of surfaces. We, however, noted that contrary to our expectation, rusty bedrails had lower levels of Aspergillus contamination. While it is generally recognised that rust promotes fungal growth and fungi contribute to acceleration of the rusting process, it has also been postulated that the excess iron in rust, the rough, porous surface, nonoptimal microenvironmental PH, and other factors could be inhibitory or toxic to fungi (25). Additional studies are necessary to better understand this relationship.
The distribution of Aspergillus species across each ward shows that surgical ward 3 had the highest Aspergillus prevalence of 55.0%. A probable reason for this high level of contamination is that samples were taken during an industrial strike by some health workers, including cleaning staff; thus only cursory cleaning was carried out. The two wards with the next highest prevalence of Aspergillus were also in this industrial action category, laying credence to our suggestion. The lack of standard and regular cleaning during this period probably encouraged accumulation of dust containing Aspergillus spores. The implication of this is an elevated risk of Aspergillosis and the potential impact on patient health and safety particularly in those with compromised immune systems. The occurrence of industrial action during this study emphasises the important role of sanitation and regular cleaning of hospital surfaces in reducing the concentration of moulds and eliminating reservoirs of Aspergillus (26).
Another compelling reason for the high contamination level observed in surgical ward 3 was that a new building was being constructed very close to the ward at the time of sample collection. It is well recognised that aerosolization and dispersal of Aspergillus species occur more commonly during or immediately after building construction or renovation activities (27). Airborne spores eventually settle on various healthcare surfaces including the bedrails. The high environmental Aspergillus created during construction and renovation activities have been linked to a higher prevalence of HAIs (28). Our study had a relatively small sample size which limited our capacity to carry out extensive statistical analysis and generate additional insights on this topic. Also, we could not assess seasonal variations in the prevalence of Aspergillus contamination due to the limited period of data collection. Further studies with larger sample sizes and longer study periods are therefore recommended. A major strength of this research is that we had the opportunity of data collection during an ongoing construction activity. This allowed us to assess the effect of such activity on Aspergillus contamination levels. We were also able to relate environmental Aspergillus to infection prevention and control (IPC), a principal approach to patient safety.
Conclusion
This study identified that Aspergillus contamination of bed rails in hospital wards is affected by environmental cleaning frequency and proximity to ongoing construction activities. We recommend strict adherence to infection prevention and control measures particularly adequate cleaning and disinfection of hospital surfaces to reduce the risk of healthcare associated Aspergillus infections.
Ethical approval
This research was approved by the University of Ibadan/ University College Hospital (UI/UCH) Ethics review board with approval number UI/EC/23/0018. Permission to collect data from the wards was obtained from the hospital management following ethical approval.
Acknowledgements
We are grateful to the Department of Medical Microbiology and Parasitology, University College Hospital, Ibadan, Nigeria, for providing laboratory processing support.
References
| 1. | Khan A, Baig K, Mehboob R. Nosocomial Infections: epidemiology, prevention, control and surveillance. Asian Pac J Trop Biomed 2017; 7(5): 478–82. doi: 10.1016/j.apjtb.2017.01.019 |
| 2. | WHO report on the burden of endemic health care-associated infection worldwide. Geneva: World Health Organization; 2011, pp. 1–40. Available from: https://www.who.int/news-room/feature-stories/detail/the-burden-of-health-care-associated-infection-worldwide [cited 21 March 2023]. |
| 3. | Eames I, Tang JW, Li Y, Wilson P. Airborne transmission of disease in hospitals. J R Soc Interface 2009; 6(6): S697–702. doi: 10.1098/rsif.2009.0407 |
| 4. | Castón-Osorio JJ, Rivero A, Torre-Cisneros J. Epidemiology of invasive fungal infection. Int J Antimicrob Agents 2008; 32(2): S103–9. doi: 10.1016/S0924-8579(08)70009-8 |
| 5. | Allegranzi B, Bagheri Nejad S, Combescure C, Graafmans W, Attar H, Donaldson L, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011; 377(9761): 228–41. doi: 10.1016/S0140-6736(10)61458-4 |
| 6. | Loeffert S, Hénaff L, Dupont D, Bienvenu A, Dananché C, Cassier P, et al. Prospective survey of azole drug resistance among environmental and clinical isolates of Aspergillus fumigatus in a French University hospital during major demolition works. J Mycol Med 2018; 28: 469–72. doi: 10.1016/j.mycmed.2018.05.007 |
| 7. | Warris A, Verweij E. Clinical implications of environmental sources for Aspergillus. Med Mycol 2005; 43(1): 859–65. doi: 10.1080/13693780400025260 |
| 8. | Iyalla C. Spectrum of aspergillosis: pathogenesis, risk factors and management. Afr J Clin Exp Microbiol 2016; 17(1): 35–45. doi: 10.4314/ajcem.v17i1.5 |
| 9. | Maschmeyer G, Haas A, Cornely OA. Invasive aspergillosis: epidemiology, diagnosis and management in immunocompromised patients. Drugs 2007; 67(11): 1567. doi: 10.2165/00003495-200767110-00004 |
| 10. | Paulussen C, Hallsworth JE, Álvarez-Pérez S, Nierman WC, Hamill PG, Blain D, et al. Ecology of aspergillosis: insights into the pathogenic potency of Aspergillus fumigatus and some other Aspergillus species. Microb Biotechnol 2017; 10(2): 296–322. doi: 10.1111/1751-7915.12367 |
| 11. | Karalti I, Colakoglu T. Isolation and Identification of Aspergillus species during one year in the hospitals. J Life Sci 2012; 6: 1220–4. |
| 12. | Diba K, Kordbacheh P, Mirhendi S, Rezaie S, Mahmoudi M. Identification of Aspergillus species using morphological characteristics. Pak J Med Sci 2007; 23: 867–72. |
| 13. | Sugui JA, Kwon-Chung KJ, Juvvadi PR, Latgé JP, Steinbach WJ. Aspergillus fumigatus and related species. Cold Spring Harb Perspect Med 2014; 5(2): a019786. doi: 10.1101/cshperspect.a019786 |
| 14. | Diba K, Jangi F, Makhdoomi K, Moshiri N, Mansouri F. Aspergillus diversity in the environments of nosocomial infection cases at a university hospital. J Med Life 2019; 12(2): 128–32. doi: 10.25122/jml-2018-0057 |
| 15. | Howel SA, Hazen KC, Brandt ME. Manual of clinical microbiology. 11th ed. Washington, DC: ASM Press; 2015. |
| 16. | Seagle EE, Williams SL, Chiller TM. Recent trends in the epidemiology of fungal infections. Infect Dis Clin North Am 2021; 35(2): 237–60. doi: 10.1016/j.idc.2021.03.001 |
| 17. | Pal M, Dave P, Manna A. Emerging role of Aspergillus flavus in humans and animal disorders. J Mycopath Res 2014; 52(2): 211–6. |
| 18. | Perlroth J, Choi B, Spellberg B. Nosocomial fungal infections: epidemiology, diagnosis and treatment. Med Mycol 2007; 45(4): 21–46. doi: 10.1080/13693780701218689 |
| 19. | Jangi F, Makhdoomi K, Moshiri N, Diba K, Mansouri F. Aspergillus diversity in the environments of nosocomial infection cases at a university hospital. J Med Life 2019; 12(2): 128–32. doi: 10.25122/jml-2018-0057 |
| 20. | Martínez-Herrera EO, Frías De-León MG, Duarte-Escalante E, Calderón-Ezquerro MDC, Jiménez-Martínez MDC, Acosta-Altamirano G, et al. Fungal diversity and Aspergillus in hospital environments. Ann Agric Environ Med 2016; 23(2): 264–9. doi: 10.5604/12321966.1203888 |
| 21. | Curtis L, Cali S, Conroy L, Baker K, Ou CH, Hershow R, et al. Aspergillus surveillance project at a large tertiary-care hospital. J Hosp Infect 2005; 59(3): 188–96. doi: 10.1016/j.jhin.2004.05.017 |
| 22. | Person AK, Chudgar SM, Norton BL, Tong BC, Stout JE. Aspergillus niger: an unusual cause of invasive pulmonary aspergillosis. J Med Microbiol 2010; 59(7): 834–8. doi: 10.1099/jmm.0.018309-0 |
| 23. | Rudramurthy SM, de Valk HA, Chakrabarti A, Meis JFGM, Klaassen CHW. High resolution genotyping of clinical aspergillus flavus isolates from india using microsatellites. PLoS One 2011; 6(1): e16086. doi: 10.1371/journal.pone.0016086 |
| 24. | Hicks JB, Lu ET, De Guzman R, Weingart M. Fungal types and concentrations from settled dust in normal residences. J Occup Environ Hyg 2005; 2(10): 481–92. doi: 10.1080/15459620500252860 |
| 25. | Parveen S, Wani AH, Shah MA, Devi HS, Bhat MY, Koka JA, et al. Preparation, characterization and antifungal activity of iron oxide nanoparticles. Microb Pathog 2018; 115: 287–92. doi: 10.1016/j.micpath.2017.12.068 |
| 26. | Anaissie E, Stratton S, Dignani M. Cleaning patient shower facilities: a novel approach to reducing patient exposure to aerosolized Aspergillus species and other opportunistic moulds. Clin Infect Dis 2002; 35(8): E86–8. doi: 10.1086/342305 |
| 27. | Cooper E, O’Reilly M, Guest D, Dharmage S. Influence of building construction work on Aspergillus infection in a hospital setting. Infect Control Hosp Epidemiol 2003; 24(7): 472–6. doi: 10.1086/502239 |
| 28. | Kanamori H, Rutala WA, Sickbert-Bennett EE, Weber DJ. Review of fungal outbreaks and infection prevention in healthcare settings during construction and renovation. Clin Infect Dis 2015; 61: 433–44. doi: 10.1093/cid/civ297 |