ORIGINAL ARTICLE
Epidemiological insights into Shigella infections in Ethiopia: a study of prevalence, antimicrobial resistance, and associated factors
Amete Mihret Teshale1,2*, Alem Abrha Kalayu1, Eyasu Tigabu Seyoum3 and Woldaregay Erku Abegaz1
1College of Health Sciences, Department of Microbiology, Immunology and Parasitology, Addis Ababa University, Addis Ababa, Ethiopia; 2National Clinical Bacteriology and Mycology Reference Laboratory, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 3The Ohio State Global One Health, Addis Ababa, Ethiopia
Abstract
Objective: The aim of this study was to assess the prevalence of Shigella infection, its antimicrobial resistance patterns, and associated risk factors among diarrheal patients in Ethiopia.
Method: A cross-sectional study was conducted from October 2021 to November 2022 among 2,331 diarrheal patients from Addis Ababa, Gondar, and Harar. Data on socio-demographics and clinical characteristics were collected using a structured questionnaire and REDCap software. Stool samples were processed using standard microbiological methods, and Shigella isolates were confirmed by polymerase chain reaction. Antibiotic susceptibility testing was performed using the Phoenix M50 machine. Data analysis was conducted in R software, employing univariable and multivariable logistic regression to identify associated factors.
Result: This study indicated that the prevalence of Shigella spp. was 2.79%, highest in Harar (5.05%) and lowest in Addis Ababa (0.88%). Being resistance to ciprofloxacin (43.08%) and azithromycin (32.31%), key antibiotics recommended for shigellosis treatment are alarmingly high across study sites. The resistance to at least one antibiotic was shown by 98.46% of the isolates, with 33.85 and 73.85% being extended-spectrum beta-lactamase (ESBL) producers and multidrug-resistant (MDR), respectively, and showed significant variation among study sites. Harar had the highest odds of Shigella infection compared to Addis Ababa [AOR: 1.39, 95% CI: 1.02, 1.57] and Gondar [AOR: 1.12, 95% CI: 1.01, 1.24], while Gondar had higher odds than Addis Ababa [AOR: 1.15, 95% CI: 1.09, 1.35]. Households with unimproved water sources and unimproved sanitation showed higher odds of Shigella infection [AOR: 1.99, 95% CI: 1.17, 3.01, P = 0.03] and [AOR: 1.39, 95% CI: 1.27, 1.74, P = 0.03], respectively.
Conclusion: In conclusion, Shigella infections in Ethiopia exhibit high ESBL and MDR rates, emphasizing the need for improved sanitation, water safety, and antibiotic stewardship.
Keywords: Shigella infection; antimicrobial resistance; prevalence; risk factors; Ethiopia
Citation: Int J Infect Control 2025, 21: 23852 – http://dx.doi.org/10.3396/ijic.v21.23852
Copyright: © 2025 Amete Mihret Teshale et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 16 May 2025; Accepted: 3 November 2025; Published: 17 April 2026
Competing interests and funding: The authors declared that there is no conflict of interest. This work was funded by the Ethiopian Public Health Institute and Addis Ababa University as a small student fund.
*Amete Mihret Teshale, Email: 2017ametemihret@gmail.com
Shigellosis, caused by the genus Shigella, is a global public health issue and a major cause of diarrhea worldwide (1). It presents challenges in food safety and health, leading to mild diarrhea or severe dysentery, with complications like electrolyte imbalance, hemolytic colitis, and hemolytic uremic syndrome (2). Moreover, the global burden of Shigella indicated an estimated 165 million cases yearly, with over 100 million in low- and middle-income countries (LMICs), resulting in over one million deaths. Studies confirm Shigella as a key cause of diarrheal morbidity in infants and young children in LMICs such as Ethiopia (3).
Shigella, a Gram-negative bacterium, comprises four species (S. dysenteriae, S. flexneri, S. boydii, and S. sonnei), each with varying virulence (4). A low infectious dose (10–100 bacteria) can cause infection (5), spreading easily in areas with poor sanitation, and peaks being during warmer months (4). In resource-limited settings, S. dysenteriae and S. flexneri are common, with S. dysenteriae type 1 causing the most severe cases due to shiga-toxin production (5). Transmission occurs via the fecal-oral route, often through contaminated food, water, or person-to-person contact in crowded environments where poor sanitation, limited access to clean water, and inadequate hygiene are critical risk factors (6).
The rise of antimicrobial resistance (AMR) among Shigella strains is an increasing public health threat, with multidrug-resistant (MDR) strains complicating treatment and prolonging illness and transmission (6). Shigella is one of the eight World Health Organization priority pathogens due to its resistance burden (7). Globally, AMR causes 700,000 deaths annually, projected to reach 10 million by 2050 if no action is taken (7).
In Ethiopia, data on Shigella’s burden across wider age groups, geographic regions, and seasons are limited, though studies focused on specific areas (8, 9) and under five children are available (9, 10). Hence, comprehensive studies on Shigella’s seasonal and regional distribution, alongside understanding variations in its prevalence and resistance, are vital for targeted interventions and effective public health strategies. This study is essential as it highlights Shigella’s dual burden as both a persistent diarrheal pathogen and a growing AMR threat among the three major cities in Ethiopia. Hence, this study aimed to estimate the prevalence of Shigella infection, its AMR patterns, and associated risk factors among diarrheal patients in Ethiopia.
Materials and methods
Study site and population
A cross-sectional study was conducted from October 2021 to November 2022 to estimate the prevalence and antibiotic susceptibility pattern of Shigella spp. among diarrheal patients submitting physician-requested stool samples to the clinical laboratories at three hospitals in Ethiopia: Yekatiti-12 Hospital, a specialized teaching hospital in Addis Ababa; University of Gondar Comprehensive Specialized Hospital, a referral and teaching Hospital in Gondar; and Hiwot Fana Comprehensive Specialized Hospital, a teaching Hospital in Harar. These study sites were selected because they serve a large and diverse population and are representative of the three predominant ecosystems in Ethiopia: central (Addis Ababa), north (Gondar), and south-eastern (Harar). These hospitals were purposefully selected because each is a major referral and teaching institution in its region with high clinical throughput and established laboratory capacity for microbiological testing, which ensured consistent specimen processing and susceptibility testing across sites. Additionally, the three sites collectively represent geographically and ecologically distinct areas of the country (central, northern, and eastern Ethiopia), allowing us to capture variation in pathogen prevalence and resistance patterns across diverse patient populations. Selection was guided by operational feasibility, the ability to obtain physician-referred stool specimens, and the intention to sample both urban and referral catchment populations to improve the generalizability of our findings.
Sample size determination and recruitment of participants
The single population proportion formula was used to calculate the sample size with the estimated population proportion of 50%, n = (Zα/2)2* p(1-p)/(e)2, where p represents population proportion (50%), Zα/2 = 1.96 at 95% confidence interval, and e = 0.025. 384 per site (three sites), per season (dry and rainy season) gives a total of 384*2 = 768 participants per site. The overall sample size becomes 768*3 = 2,304.
Patients were eligible to participate in the study if they were ordered by their physician to provide a stool sample for testing, had diarrhea, had not taken antibiotics in the last 2 weeks, and lived in the defined catchment area of the hospital. The catchment areas for the three hospitals were defined using information from the local health bureaus in relation to where individuals typically seek medical care.
Patient consent statement
Eligible patients were recruited to participate in the study when they consecutively arrived at the clinical laboratory, and a written informed consent was obtained. Parental consent was obtained for children under the age of 18, and assent was also obtained from children aged 12–17 years. Following consent, participants completed a pre-tested survey via an interview with a trained study team member. The survey included questions about socio-demographic characteristics (e.g. age and sex); monthly household income; the current diarrheal illness (e.g. symptoms); and environmental exposures (e.g. animal and water).
Stool sample collection
Stool samples were obtained according to the physician’s instructions and tested for Shigella spp. using standardized protocols that included bacterial culture, biochemical tests, and polymerase chain reaction (PCR). Submitted stool samples were screened and excluded if the sample was unlabeled or mislabeled, received in a non-sterile stool collection cup, or leaking container. Samples collected at a location other than the microbiology laboratory (e.g. parasitology laboratory) were transferred to Cary-Blair transport media and transported to the testing microbiology laboratories within 4 h of collection using a cold-chain transportation system.
Culture, identification, and PCR confirmation
Stool samples were placed in Selenite-F broth using a 10 µL plastic loop and incubated at 35±2°C overnight (11). Enriched broth was inoculated on MacConkey (MAC, Difco, USA) and Xylose-Lysine-Deoxycholate (XLD, Difco, USA) agar and then incubated at 35 ± 2°C overnight. Colonies were examined for Shigella characteristics: small, reddish, moist colonies on XLD (Difco, USA) and non-lactose fermenting colonies on MAC (Difco, USA). Biochemical analyses were conducted using Triple Sugar Iron Agar (TSIA, Difco, USA), Lysine Iron Agar (LIA, Difco, USA), Simmon Citrate Agar (SCA, Difco, USA), Urease Agar (UA, Difco, USA), and Sulfide Indole Motility Agar (SIMA, Difco, USA) with identification based on standard biochemical features. All samples and biochemical analysis were incubated at 35 ± 2 °C overnight in calibrated thermostatic incubators. Internal temperature was verified daily with an independent thermometer, and records were maintained as part of laboratory quality assurance. Any deviation outside the acceptable range was corrected immediately to ensure consistent incubation conditions.
Molecular confirmation targeted the ipaH gene using PCR (12). DNA was extracted using the boiling method (13): colonies were suspended in nuclease-free water, centrifuged, and resuspended in 250 µL nuclease-free water and then boiled, cooled, and centrifuged. The supernatant served as the DNA template and was measured using NanoDrop 2000 (14). Monoplex PCR was conducted following a prior protocol (15), with 95°C initial denaturation for 3 min, followed by 45 cycles at 95°C for 15 sec and annealing/extension at 60°C for 30 sec. The forward primer (ipaHF:5’-ACCATGCTCGCAGAGAAACT-3’), reverse primer (ipaHR: 5’ TACGCTTCAGTACAGCATGC-3’), and TaqMan probe (ipaHP:5’- [CAL Flour Red 610]-TGGCGTGTCGGGAGTGACAGC-[BHQ-2]-3’) were used. All the ipaH gene positive Shigella isolates were tested for lacY gene to differentiate it from the closely related bacteria Enteroinvasive Escherichia coli (EIEC). The absence of lacY in our isolates confirmed the specificity of the ipaH-based Monoplex PCR for Shigella spp. The forward primers (lacYF: ACCAGACCCAGCACCAGATAAG), reverse primers (lacYR: CTGCTTCTTTAAGCAACTGGCGA), and probe (lacYP: FAM-CATACATATTGCCCGCCAGTACAGAC-BBQ) were used (16). A 181-bp PCR amplicon was expected in the presence of the Shigella-specific ipaH gene and the absence of the lacY gene in our Shigella spp.
Antimicrobial susceptibility testing
The AST was performed using the Phoenix M50 machine obtained from Becton Dickinson (BD, USA), according to the manufacturer’s instructions (17). Each isolate was tested for penicillin, quinolones, tetracycline, folate-pathway antagonists, cephalosporins, macrolides, and carbapenems. Sulfamethoxazole-trimethoprim is the only folate-pathway antagonist tested. Moreover, the BD Phoenix extended-spectrum beta-lactamase (ESBL) test was used to screen for ESBL production, followed by phenotypic confirmation using the double disc diffusion method (18).
Data analysis
Descriptive statistics were used to summarize socio-demographic characteristics, symptoms, and laboratory test results. The prevalence of Shigella spp. and the respective 95% confidence intervals were calculated using the binomial proportion test and logistic regression. Seasonal trends of Shigella spp. were assessed overall by month and by study site. Risk factors such as sex, age, residence (urban vs. rural), season, sanitation facilities, water sources of the household, and domestic animals’ ownership for a positive laboratory test result were identified for each study site separately using univariable and multivariable logistic regression. Initially, the season was classified as rainy or dry, but, due to changing weather patterns, it was re-classified in the analysis as dry (October to February), short rain (March to May), and long rain (June to September) (19). Water sources and sanitation facilities were classified as improved or unimproved based on established WHO/UNICEF Joint Monitoring Programme standards (20). Data were collected electronically using REDCap (National Center for Advancing Transnational Sciences, Grant UL1TR001070) (21) and analyzed using R (R Core Team 2021) (22).
Results
Socio-demographic conditions, clinical factors, and the occurrence of Shigella
A total of 2,331 patients were enrolled in the study (Table 1). Ages ranged from 2 months to 94 years, with a mean age of 29.83 years (SD+19.85). All participants from Addis Ababa were urban residents, while about a quarter of participants from Harar and Gondar lived in rural areas. Most participants (1,277, 54.78%) in all study sites were male. Monthly household income varied with Addis Ababa having the lowest income (<2,000 birr) compared to Gondar (8,000–10,000 birr) and Harar (6,000–8,000 birr). About half of the study participants were enrolled during the dry season. Abdominal pain and abdominal cramps were the most reported symptoms, and watery stool was the most common type of stool reported.
| Characteristics | Categories | Addis Ababa n (%) | Gondar n (%) | Harar n (%) | Overall n (%) | Shigella spp. n (%) | Prevalence (95%CI) |
| Total Patients | 792 (33.98) | 767 (32.90) | 772 (33.11) | 2,331 (100) | 65 (100) | 2.79 (2.19, 3.54) | |
| Age group (years) | <5 | 99 (12.50) | 124 (16.17) | 105 (13.60) | 328 (14.07) | 10 (15.38) | 3.05 (1.66, 5.52) |
| 5–14 | 53 (6.69) | 96 (12.52) | 79 (10.23) | 228 (9.78) | 6 (9.23) | 2.63 (1.21, 5.62) | |
| 15–19 | 30 (3.79) | 47 (6.13) | 30 (3.89) | 107 (4.59) | 4 (6.15) | 3.74 (1.46, 9.22) | |
| 20–29 | 144 (18.18) | 205 (26.73) | 199 (25.78) | 548 (23.51) | 23 (35.38) | 4.20 (2.81, 6.22) | |
| 30–39 | 123 (15.53) | 125 (16.30) | 164 (21.24) | 412 (17.67) | 8 (12.31) | 1.94 (0.99, 3.78) | |
| 40–49 | 111 (14.02) | 81 (10.56) | 106 (13.73) | 297 (12.74) | 8 (12.31) | 2.69 (1.37, 5.22) | |
| 50+ | 232 (29.29) | 89 (11.60) | 89 (11.53) | 411 (17.63) | 6 (9.23) | 1.46 (0.67, 3.15) | |
| Sex | Male | 410 (51.77) | 432 (56.32) | 435 (56.35) | 1,277 (54.78) | 33 (50.77) | 2.58 (1.85, 3.61) |
| Female | 382 (48.23) | 335 (43.68) | 337 (43.65) | 1,054 (45.22) | 32 (49.23) | 3.04 (2.16, 4.25) | |
| Residence | Urban | 792 (100.00) | 596 (77.70) | 573 (74.22) | 1,961 (84.13) | 55 (84.62) | 2.80 (2.16, 3.63) |
| Rural | 0 (0.00%) | 171 (22.30) | 199 (25.78) | 370 (15.87) | 10 (15.38) | 2.70 (1.47, 4.90) | |
| Monthly Household Income (ETB) | <2,000 | 203 (25.63) | 109 (14.21) | 30 (3.89) | 342 (14.67) | 4 (6.15) | 1.17 (0.46, 2.97) |
| 2,000–4,000 | 195 (24.62) | 49 (6.39) | 108 (13.99) | 352 (15.10) | 6 (9.23) | 1.70 (0.78, 3.67) | |
| 4,000–6,000 | 124 (15.66) | 54 (7.04) | 116 (15.03) | 294 (12.61) | 10 (15.38) | 3.40 (1.86, 6.15) | |
| 6,000–8,000 | 114 (14.39) | 89 (11.60) | 200 (25.91) | 403 (17.29) | 12 (18.46) | 2.98 (1.71, 5.13) | |
| 8,000–10,000 | 47 (5.93) | 204 (26.60) | 157 (20.34) | 408 (17.50) | 15 (23.08) | 3.68 (2.24, 5.98) | |
| >10,000 | 20 (2.52) | 114 (14.86) | 32 (4.15) | 166 (7.12) | 2 (3.08) | 1.20 (0.33, 4.29) | |
| Unknown | 89 (11.24) | 148 (19.30) | 129 (16.71) | 366 (15.70) | 16 (24.62) | 4.37 (3.13, 7.64) | |
| Season | Dry | 435 (54.92) | 365 (47.59) | 341 (44.17) | 1,141 (48.95) | 32 (49.23) | 2.80 (1.99, 3.93) |
| Short Rains | 127 (16.04) | 257 (33.51) | 142 (18.39) | 526 (22.57) | 19 (29.23) | 3.61 (2.32, 5.57) | |
| Long Rains | 230 (29.04) | 145 (18.90) | 289 (37.44) | 664 (28.49) | 14 (21.54) | 2.11 (1.49, 3.88) | |
| Types of stools* | Watery stool | 370 (46.72) | 628 (81.88) | 624 (80.83) | 1,622 (69.58) | 55 (84.62) | 3.39 (2.61, 4.39) |
| Bloody stool | 30 (3.79) | 197 (25.68) | 60 (7.77) | 287 (12.31) | 10 (15.38) | 3.48 (1.90, 6.29) | |
| Mucoid stool | 61 (7.70) | 269 (35.07) | 100 (12.95) | 430 (18.45) | 12 (18.46) | 2.79 (1.60, 4.81) | |
| Sign and Symptoms* | Abdominal cramps | 352 (44.44) | 535 (69.75) | 470 (60.88) | 1,357 (58.22) | 38 (58.46) | 2.80 (2.05, 3.82) |
| Undefined Abdominal pain | 426 (53.79) | 541 (70.53) | 567 (73.45) | 1,534 (65.81) | 47 (72.31) | 3.06 (2.31, 4.05) | |
| Fever | 166 (20.96) | 345 (44.98) | 301 (38.99) | 812 (34.83) | 28 (43.08) | 3.45 (2.40, 4.94) | |
| Nausea | 218 (27.53) | 66 (8.60) | 106 (13.73) | 390 (16.73) | 1 (1.54) | 0.44 (0.08, 2.46) | |
| Vomiting | 122 (15.40) | 141 (18.38) | 181 (23.45) | 444 (19.05) | 9 (13.85) | 2.03 (1.22, 4.33) | |
| Bloating | 178 (22.47) | 41 (5.35) | 7 (0.91) | 226 (9.70) | 8(24.62) | 3.53 (2.23, 5.77) | |
| None | 11 (1.39) | 9 (1.17) | 8 (1.04) | 28(1.20) | 1(58.46) | 3.57 (2.05, 3.82) | |
| Household water sources | Improved | 730 (92.17) | 612 (79.79) | 543 (70.34) | 1,885 (80.87) | 52 (80.00) | 2.76 (2.20, 3.72) |
| Unimproved | 62 (7.83) | 155 (20.21) | 229 (29.66) | 446 (19.13) | 13 (20.00) | 2.91 (1.71, 4.92) | |
| Toilet types | Improved sanitation | 555 (70.08) | 483 (62.97) | 625 (80.96) | 1,663 (71.34) | 44 (67.69) | 2.65 (2.18, 3.81) |
| Unimproved sanitation | 237 (29.92) | 284 (37.03) | 147 (19.04) | 668 (28.66) | 21 (32.31) | 3.14 (1.83, 4.40) | |
| Availability of animals | Cattle | 22 (2.78) | 49 (6.39) | 183 (23.70) | 254 (10.90) | 12 (18.46) | 4.72 (2.72, 8.07) |
| Sheep | 14 (1.77) | 30 (3.91) | 63 (8.16) | 107 (4.59) | 4 (6.15) | 3.74 (1.46, 9.22) | |
| Goat | 8 (1.01) | 11 (1.43) | 126 (16.32) | 145 (6.22) | 7 (10.77) | 4.83 (2.36, 9.63) | |
| Chickens | 16 (2.02) | 22 (2.87) | 123 (15.93) | 161 (6.91) | 6 (9.23) | 3.73 (1.72, 7.89) | |
| Dog_Cat | 108 (13.64) | 72 (9.39) | 56 (7.25) | 236 (10.12) | 8 (12.31) | 3.39 (1.73, 6.55) | |
| *Patients could have multiple types of stools and/or symptoms. ETB: Ethiopian birr. Improved water sources: household connections such as piped houses, piped yards, public standpipes, boreholes, protected dug wells, protected springs, and rainwater collection. Unimproved water sources: unprotected wells, unprotected springs, surface water, and tanker truck-provided water. Improved sanitation: flush to sewer system, flush to septic tank, and pit-latrine with cover. Unimproved sanitation: pit-latrine without cover, open defecation. | |||||||
Culture-based identification detected Shigella spp. in 3.13% (73/2,331) of samples, while PCR confirmed 2.79% (65/2,331). The overall prevalence of Shigella spp. was 2.79% [95% CI: 2.19, 3.54], varying by demographic, environmental, and health factors (Table 1). Harar had the highest prevalence at 5.05% [95% CI: 3.71, 6.83], followed by Gondar, 2.48% [95% CI: 1.59, 3.84], and Addis Ababa, the lowest at 0.88% [95% CI: 0.43, 1.81]. Participants aged 20–29 years had the highest prevalence at 4.20% [95% CI: 2.81, 6.22], while those 50+ years had the lowest at 1.46% [95% CI: 0.67, 3.15]. Prevalence was slightly higher in urban areas, 2.80% [95% CI: 2.16, 3.63], than rural residents. Females had a slightly higher prevalence, 3.04% [95% CI: 2.16, 4.25], than males. Households with unknown monthly income had the highest prevalence at 4.37% [95% CI: 3.13, 7.64]. Watery diarrhea was the most common symptom with Shigella spp. prevalence at 3.39% [95% CI: 2.61, 4.39].
Household water sources, sanitation facilities, and animal ownership varied across the study sites, with unimproved water sources being found overall (19.13%), Harar having the highest proportion (29.66%), and the lowest in Addis Ababa (7.83%) (Table 1). The overall availability of unimproved sanitation facilities was 28.66%, with Gondar showing slightly higher (37.03%), followed by Addis Ababa (29.92%) (Table 1). Shigella prevalence was higher among those with unimproved water, 2.91% [95% CI: 1.71, 4.92], and unimproved sanitation, 3.14% [95% CI: 1.83, 4.40]. Moreover, Harar had the highest ownership of animals, including cattle (23.70%), goats (16.32%), and chickens (15.93%), which were associated with an overall higher Shigella prevalence, particularly among goats, 4.83% [95% CI: 2.36, 9.63], and cattle, 4.72% [95% CI: 2.72, 8.07]. Watery diarrhea was the most common type of stool among participants with Shigella spp. prevalence, at the rate of 3.39% [95% CI: 2.61, 4.39]. Among the signs and symptoms, participants with vomiting, 3.60% [95% CI: 2.23, 5.77], and fever, 3.57% [95% CI: 2.40, 4.94], showed high prevalence of Shigella spp. (Fig. 1).
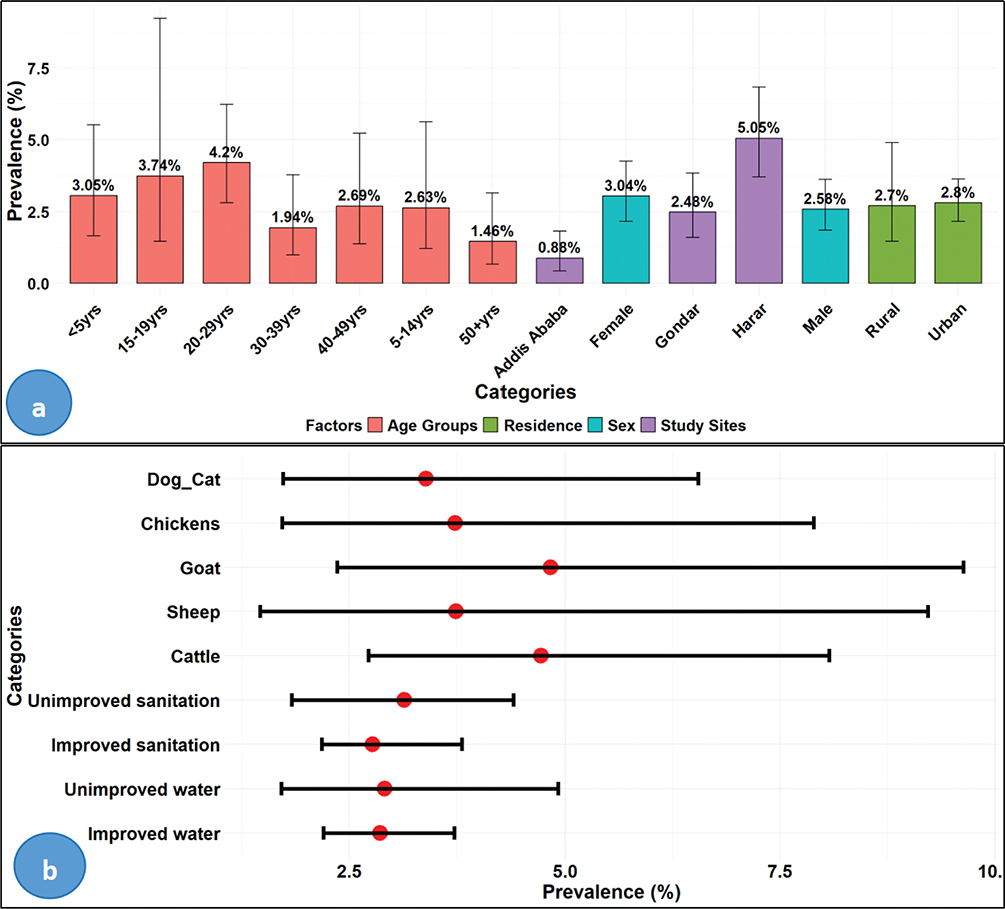
Fig. 1. Prevalence with 95% confidence interval of Shigella spp. by socio-demographic (A) and environmental factors (B). Note: yrs: years.
Seasonal variation in Shigella isolation rates
The overall seasonal prevalence of Shigella peaked during the short rainy season, 3.61% [95% CI: 2.32, 5.57], and the least was during the long rainy season, 2.11% [95% CI: 1.49, 3.88] (Table 1). Moreover, the monthly distribution of Shigella spp. showed the highest proportion in warmer months of the year, such as February (5.75%), followed by May (4.73%) and March (4.35%), with notable variations across the study sites (Figure 2). For instance, Harar showed the highest proportion, particularly in February (12.77%) and December (9.35%). Gondar showed a significant rise in February (4.92%) and September (5.56%). In contrast, Addis Ababa maintained an overall lower proportion, with a peak in July (4.71%).
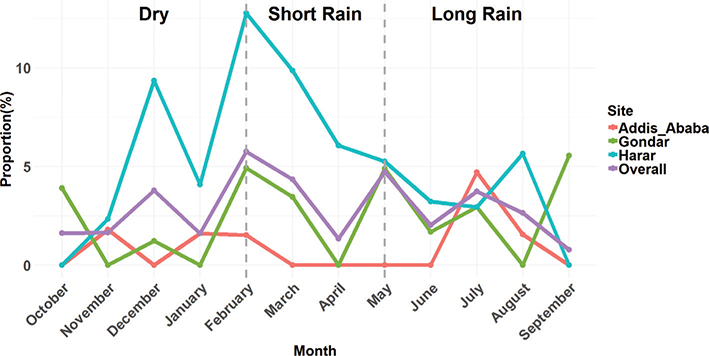
Fig. 2. Monthly trends of Shigella spp. by study sites.
Antimicrobial resistance patterns among Shigella isolates
The antibiotic resistance profiles of Shigella spp. varied among the three regions (Figure 3A). For antibiotics recommended for the treatment of Shigella spp., resistance patterns revealed significant variability across study sites. Ciprofloxacin, a frontline treatment, showed an overall resistance at 43.08% (28/65), with the highest resistance in Addis Ababa, 71.43% (5/7), and the lowest in Gondar, 31.58% (6/19). Azithromycin resistance was 32.31% (21/65) overall, with similar patterns across sites, ranging from 21.05% (4/19) in Gondar to 30.77% (12/39) in Harar. Notably, ceftriaxone exhibited 38.46% (25/65) resistance overall, with slightly higher resistance, 42.1% in Addis Ababa (3/7) and Gondar (8/19) each than in Harar, 35.9% (14/39). Furthermore, the only folate-pathway antagonist tested in our study, that is, sulfamethoxazole-trimethoprim (SXT), was found resistance in 60% of the Shigella isolates. The regional distribution indicated that Addis Ababa showed the highest proportion, 71.43%, followed by Harar, 61.54%, and the slightly lower proportion was reported in Gondar, 52.63%. Importantly, no resistance to meropenem was observed across all sites, 0%, indicating that this agent retained full activity against all Shigella isolates tested in this study. The overall proportion of MDR was 73.85% (48/65) with variation among study sites. For example, the highest proportion was found in Addis Ababa, where 85.71% (6/7) of the Shigella spp. were found as MDR, followed by Harar, 76.92% (30/39), and Gondar, 63.16% (12/19). Moreover, the overall proportion of ESBL-producing Shigella spp. was found to be 33.85% (22/65), which significantly varied by study sites (Figure 3B). The proportion of ESBL was highest in Addis Ababa, 71.43% (5/7), followed by Harar, 35.90% (14/39).
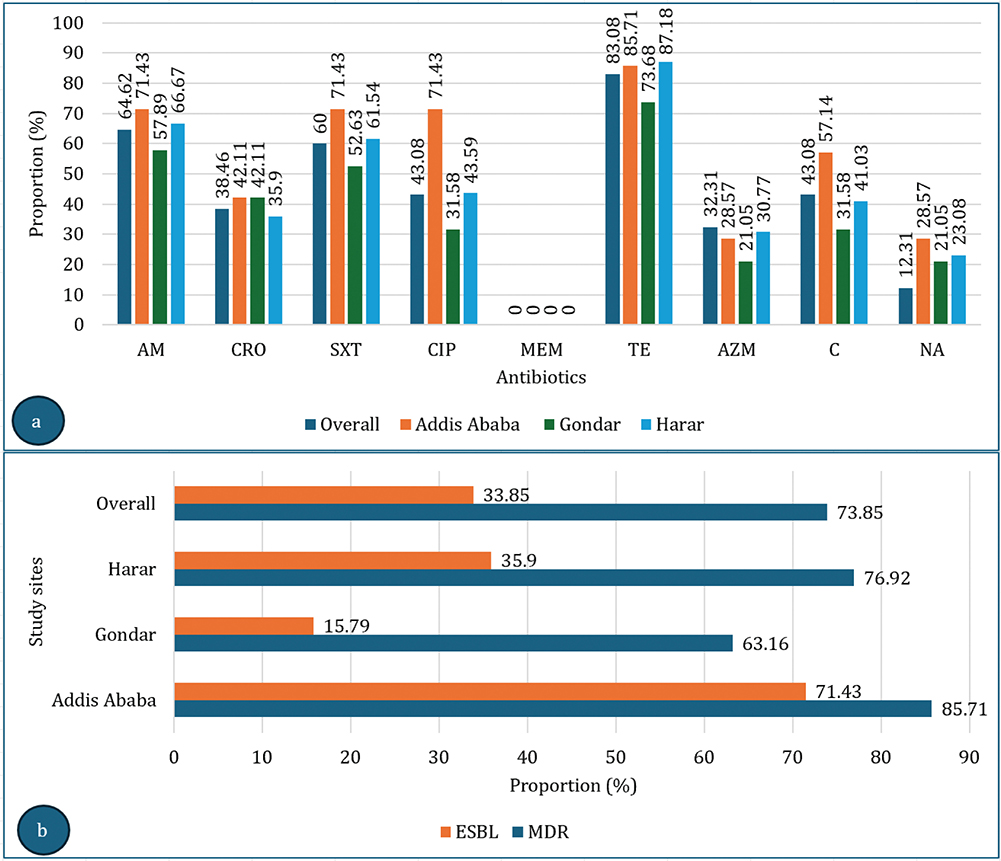
Fig. 3. Antibiotic resistance patterns (%) of Shigella spp. among study sites for the antibiotics recommended for the treatment of diarrhea (A) and proportion of ESBL and MDR (B). Note the denominator for the overall ESBL and MDR is the 65 Shigella spp., but the denominator for the study sites was the number of Shigella spp. for each study sites (7, 19, and 39 for Addis Ababa, Gondar, and Harar, respectively). Note: AZM: Azithromycin; C: Chloramphenicol; NA: Nalidixic Acid; AM: Ampicillin; CRO: Ceftriaxone; SXT: Sulfamethoxazole-trimethoprim; CIP: Ciprofloxacin; MEM: Meropenem; TE: Tetracycline; ESBL: Extended-spectrum beta-lactamase; MDR: Multidrug resistance.
Associated factor for Shigellosis
In univariable analysis, age, study sites, and environmental factors were associated with Shigella infection (Table 2). In the multivariable analysis, living in Harar (AOR: 1.39, 95% CI: 1.02, 1.57, P = 0.00) and Gondar (AOR: 1.15, 95% CI: 1.09, 1.35, P = 0.04) remained significantly associated with higher odds of infection compared to Addis Ababa. Unimproved water sources (AOR: 1.99, 95% CI: 1.17, 3.01, P = 0.03) and unimproved sanitation (AOR: 1.39, 95% CI: 1.27, 1.74, P = 0.03) were strongly associated with increased odds of infection (Table 2).
Discussion
Shigella infections remain a major public health concern, particularly in LMICs, such as Ethiopia, where key risk factors such as poor sanitation, unsafe water, and overcrowded living conditions are prevalent (23, 24), leading to increased morbidity and mortality. Most studies on Shigella in Ethiopia are geographically and seasonally limited (8–10), restricting comprehensive assessments of its distribution. Our study addresses these gaps by covering a wider geographic area over an entire year, providing valuable insights into Shigella prevalence and distribution across regions and seasons in Ethiopia. Moreover, our study conducted the assessment of the wider types of antibiotics that can show the antibiotic resistance pattern of Shigella to the antibiotics that are not commonly prescribed for the treatment of diarrheal illness, and the burden of AMR among the Shigella spp. in Ethiopia.
In addition, previous studies primarily used culture and biochemical methods alone (8, 10), which have variable sensitivity and specificity, complicating reliable differentiation from genetically similar organisms like E. coli (EIEC). Even the molecular methods, such as 16S rRNA sequencing, face challenges in this regard (25). Besides, earlier studies mostly focused on children under five (9, 10), and information related to other age groups is limited. Our research included individuals with all ages and found the highest prevalence in individuals aged 20–29 years (4.20%) compared to 3.05% in children under five, emphasizing the need to evaluate all demographics.
In this study, the overall Shigella prevalence was found to be 2.79%, lower than the rate from meta-analyses that reported 6.6% across 29 studies in Ethiopia (3), 6.24% (26) across 43 studies in Ethiopia, and 4.0% (10) among children under 5 years in Addis Ababa, Ethiopia. These discrepancies may have resulted from the conventional identification methods used in those studies included in the aforementioned meta-analyses, which could overestimate prevalence. Site-specific results showed that Addis Ababa exhibited the lowest prevalence (0.88%), likely due to urban residents having better access to healthcare and food safety information (23, 24), unlike rural Ethiopians, where, for example, 56% of whom still use unimproved toilet facilities (27). However, another meta-analysis reflecting the findings of health facility and community studies found a higher (2.2%) prevalence in Addis Ababa (3). Some more prospective studies also reported higher prevalence rates, such as 5.6% (8) and 8.8% (10). Those higher prevalence rates indicated in the latter reports could be due to the recruitment of study participants from health centers where active cases are accessed easily, which potentially may have skewed the results.
Similarly, our finding in Northern Ethiopia (Gondar) revealed a 2.48% prevalence, which is notably lower than previous reports of 4.57% (28), 15.6% (25), and 10.7% (29). Seasonal factors likely influenced these differences, as the latter studies were conducted during the dry seasons only, during which Shigella prevalence tends to rise. This highlights the importance of considering seasonal variations when interpreting epidemiological data, as they can significantly impact reported prevalence rates. In Eastern Ethiopia (Harar), we found a 5.05% prevalence, consistent with a 5.6% prevalence in Dire Dawa (30), but a bit higher than a recent study reporting 2.5% in Jigjiga (31) and significantly lower than an earlier report of 14.6% in Jigjiga (32). The higher prevalence observed in our study may be attributed to year-round data collection, covering dry, short rainy, and long rainy seasons, which captures the overall burden of Shigella infection. In contrast, the study in Jigjiga (32) was conducted over a short 2-week period during the short rainy season and may not have included the dry season, when water shortages and compromised sanitation can increase the risk of Shigella transmission, which was found in our study. Additionally, disparities in water access likely contributed to these differences, with 81% of Jigjiga households relying on substandard sources (33), which could increase the risk of Shigella transmission.
Significant overall prevalence fluctuations of Shigella spp. were observed across the three seasons, peaking during the dry season (3.61%) followed by the short rainy season (2.11%), indicating the environmental factors’ influence over Shigella transmission. For instance, higher rates during the dry season correlate with compromised water quality and sanitation (34). Similar seasonal patterns have been observed in East Africa, with outbreaks peaking during drier periods due to water scarcity and increased exposure to contaminated environments (35).
Shigella treatment typically includes azithromycin, ciprofloxacin, ceftriaxone, trimethoprim-sulfamethoxazole, and ampicillin, but due to rising AMR, the WHO recommends fluoroquinolones as the first-line therapy and β-lactams and cephalosporins as second-line options (36). In areas with high ciprofloxacin resistance, azithromycin is also suggested as the second-line treatment, whereas ampicillin, chloramphenicol, co-trimoxazole, tetracyclines, and nalidixic acid are discouraged due to widespread resistance (37). In our study, 98.46% of Shigella isolates exhibited resistance to at least one antibiotic, particularly to first-line treatments, a considerably higher rate than the 50% resistance reported by Hussen et al. [3]. This elevated resistance level presents significant challenges to clinical management, especially in Ethiopia, where healthcare access is often constrained.
The notably high resistance to tetracycline was above 80% in Addis Ababa and Harar. In Addis Ababa, almost half of the tested antibiotics, which include the first line of antibiotics, that is, ciprofloxacin, showed resistance to greater than 70%. Additionally, more than three types of antibiotics, such as tetracycline, showed the resistance of greater than 60% in Harar. This is higher than the reported resistance rates to ciprofloxacin (29.8%), azithromycin (29.2%), and ceftriaxone (23.8%) in another study (38). The differences in resistance levels may be attributed to variations in antibiotic use and access among different geographies. Furthermore, azithromycin, the antibiotics used for severe disease, showed an overall resistance of greater than 30%, with a very close burden among the different study sites. Similarly, this increased resistance to azithromycin across the study sites suggests widespread use of this antibiotic, which could be contributing to the rise in resistance. This warrants closer monitoring and cautious use of this antibiotic to preserve its efficacy. Interestingly, none of the Shigella isolates in our study was resistant to meropenem, aligning with its restricted use as a last-line treatment. This is consistent with data from a systematic review of 63 studies conducted between 2010 and 2022 in Asian countries, where resistance to meropenem was almost non-existent (38).
Additionally, 33.85% of all the isolates across the study sites were found to be ESBL-producing. Notably, Addis Ababa had the highest ESBL rate (71.43%), nearly five times higher than that in Gondar (15.79%) and double those observed in Harar (35.90%). Additionally, the MDR of Shigella spp. is increasingly recognized as of significant concern in developing countries, especially in Africa, and an escalating public health concern. In this study, the overall MDR rate was 73.85%, which is closer to the findings of a meta-analysis of 43 studies that reported an MDR of 79.08% (39). The consistency between our findings and those from the meta-analysis suggests that MDR remains a widespread issue in Ethiopia, further emphasizing the urgency of implementing targeted antimicrobial stewardship interventions. Regional differences in MDR rates were evident in our study, with Addis Ababa exhibiting the highest MDR (85.71%), followed by Harar (76.92%) and Gondar (63.16%).
Among the associated factors assessed, study sites significantly influence Shigella prevalence in Ethiopia, with Harar having the odds of 1.39 compared to Addis Ababa. Moreover, Harar had the odds of 1.12 than Gondar, and Gondar had the odds of 1.15 for Shigella infection compared to Addis Ababa. This prevalence variation seems to be largely influenced by environmental factors, including water sources and sanitation practice, where populations relying on unimproved water sources and shared latrines have increased the risk of Shigella infection (31). For example, in Harar, a noticeable proportion of the households relied on unimproved water sources and unimproved sanitation facilities, which might significantly correlate with a high prevalence of Shigella spp. (5.05%) in the region compared to other sites. Unimproved water sources are associated with higher microbial contamination, increasing the risk of waterborne diseases, including Shigella spp. infections, as documented in low-resource settings worldwide (40). Additionally, the high ownership of domestic animals in Harar, such as cattle and goats, might contribute to the increased burden of Shigella spp. infection, as livestock proximity can increase environmental contamination and facilitate the transmission of Shigella spp. through fecal-oral routes, which was supported by studies linking animal contact with increased risks of enteric infections (41).
In general, this study provides valuable insights into Shigella prevalence in Ethiopia, but certain limitations exist. First, our study population was limited to diarrhea patients submitting stool samples to hospitals, which may not reflect the general population’s prevalence because individuals seeking medical care are likely to have severe symptoms, potentially skewing detection rates. Second, the findings may not be generalizable to other populations and regions due to the study’s focus only on three cities in a country, and variability of risk factors, healthcare access, and pathogen prevalence among the different regions may limit the applicability of our results for the whole country. Third, healthcare-seeking behavior may have shifted during the COVID-19 pandemic, with individuals potentially avoiding hospitals due to COVID-19 fears, introducing bias. Fourth, hospital selection may introduce access-related bias, with rural patients possibly lacking access to specialized care, affecting case diversity in our study. Fifth, the financial constraints hinder us from detailing the molecular characterization of Shigella spp. to identify the circulating species, virulence factors, and antibiotic-resistant genes. Despite these limitations, our study still offers important new insights into the epidemiology of Shigella in Ethiopia.
In conclusion, our study identified regional and seasonal variations in Shigella prevalence, with Addis Ababa showing the lowest rates compared to Harar and Gondar. Moreover, the observation that rising antibiotic resistance includes the first-line antibiotics, such as ciprofloxacin, and the antibiotics that are used for severe infections, such as azithromycin. Although Shigella prevalence was lower in Addis Ababa compared to other study sites, the isolates from this major urban center exhibited higher resistance rates. This may be due to greater antibiotic use and selective pressure in urban populations, combined with improved sanitation reducing overall infection rates, highlighting that prevalence and resistance are influenced by different, though related, factors. In addition, significant ESBL and MDR strains with notable regional differences were among the important findings of this study. Furthermore, environmental factors, such as sanitation facilities, water sources, and availability of some domestic animals, were found to be significantly associated with higher odds of Shigella infection, underscoring the need for targeted public health interventions. This study highlights the urgent need for targeted public health interventions to address the regional and seasonal variation in Shigella prevalence and resistance. Hence, we recommended that, in high-prevalence regions such as Harar and Gondar, investment in sanitation infrastructure and access to clean water should be prioritized to minimize environmental transmission. Moreover, the detection of MDR and ESBL-producing strains requires the strengthening of antibiotic stewardship programs and strict adherence to WHO-recommended treatment guidelines for shigellosis. Establishing routine, seasonally focused surveillance systems is necessary to monitor both prevalence and resistance trends, enabling rapid public health response during peak transmission periods. Treatment regimens in areas with high resistance should rely on empirically effective agents such as fluoroquinolones or cephalosporins, while azithromycin should be reserved for confirmed ciprofloxacin-resistant cases. In addition, community-level education on hygiene, safe water handling, and reducing risky contact with domestic animals should be implemented to lower the burden of infection. These combined strategies of sanitation improvement, antimicrobial stewardship, continuous surveillance, and health education are essential for reducing the impact of Shigella in Ethiopia.
Acknowledgements
We would like to express our sincere gratitude to the employees at Addis Ababa University, Ethiopian Public Health Institute, Yekatit-12 Hospital, University of Gondar Hospital, and Hiwot Fana Hospital. Moreover, we would like to acknowledge the study participants whose invaluable contributions made this work possible. We would also like to express our sincere appreciation to Dr. Mohammed Ahmed for his valuable contribution in creatively designing the study site map used in this research.
Authors contribution
Amete Mihret Teshale: Methodology, Project administration, Data curation, Investigation, Formal analysis, Software, Visualization, Writing – Original draft preparation. Woldaregay Erku Abegaz: Supervision, Data curation, Validation, Formal Analysis, Writing – Review and editing, Alem Abrha Kalayu: Supervision, Methodology, Writing – Review and editing. Eyasu Tigabu: Methodology, Writing – Review and editing.
Ethical approval
Ethical approvals were obtained from the Ethiopian Public Health Institute (Protocol EPHI-IRB-311-2020) and the Addis Ababa University College of Health Sciences Institutional Review Board (Protocol 075/21/DMIP). Support letters were obtained from Yekatit-12 Hospital, Gondar Comprehensive Specialized Hospital, and Hiwot Fana Comprehensive Specialized University Hospital.
References
| 1. | Tai AYC, Easton M, Encena J, Rotty J, Valcanis M, Howden BP, et al. A review of the public health management of shigellosis in Australia in the era of culture-independent diagnostic testing. Aust N Z J Public Health 2016; 40(6): 588–91. doi: 10.1111/1753-6405.12590 |
| 2. | Bennish ML, Ahmed S. Shigellosis. In: Hunter’s tropical medicine and emerging infectious diseases. 10th ed. Elsevier; 2020, pp. 492–9. |
| 3. | Hussen S, Mulatu G, Yohannes Kassa Z. Prevalence of Shigella species and its drug resistance pattern in Ethiopia: a systematic review and meta-analysis. Ann Clin Microbiol Antimicrob 2019; 18: 1–10. doi: 10.1186/s12941-019-0321-1 |
| 4. | Puzari M, Sharma M, Chetia P. Emergence of antibiotic resistant Shigella species: a matter of concern. J Infect Public Health 2018; 11(4): 451–4. doi: 10.1016/j.jiph.2017.09.025 |
| 5. | Taneja N, Mewara A. Shigellosis: epidemiology in India. Indian J Med Res 2016; 143(5): 565–76. doi: 10.4103/0971-5916.187104 |
| 6. | Kotloff KL, Riddle MS, Platts-Mills JA, Pavlinac P, Zaidi AKM. Shigellosis. Lancet 2018; 391(10122): 801–12. doi: 10.1016/S0140-6736(17)33296-8 |
| 7. | World Health Organization. WHO bacterial priority pathogens list, 2024: bacterial pathogens of public health importance to guide research, development and strategies to prevent and control antimicrobial resistance. Geneva: WHO; 2024. Available from: https://www.who.int/publications/i/item/9789240093461 [cited 25 September 2024]. |
| 8. | Ararsa T, Wolde D, Alemayehu H, Bizuwork K, Eguale T. Prevalence and antimicrobial susceptibility profile of Salmonella and Shigella among Diarrheic patients attending selected health facilities in Addis Ababa, Ethiopia. Can J Infect Dis Med Microbiol 2023; 2023: 1–7. doi: 10.1155/2023/6104416 |
| 9. | Assefa A, Girma M. Prevalence and antimicrobial susceptibility patterns of Salmonella and Shigella isolates among children aged below five years with diarrhea attending Robe General Hospital and Goba Referral Hospital, Southeast Ethiopia. Trop Dis Travel Med Vaccines 2019; 5(1): 1–7. doi: 10.1186/s40794-019-0096-6 |
| 10. | Ayele B, Mekonnen Z, Tessema TS, Adamu E, Tsige E, Beyene G. Antimicrobial susceptibility patterns of Shigella species among children under five years of age with diarrhea in selected health centers, Addis Ababa, Ethiopia. Can J Infect Dis Med Microbiol 2023; 2023: 1–6. doi: 10.1155/2023/5379881 |
| 11. | Garcia LS. Clinical microbiology procedures handbook. 3rd ed. Vol. 1. Washington, DC: American Society for Microbiology; 2008, pp. 3.8.1.1–3.8.5.4. |
| 12. | Bio Molecular Systems (BMS). Magnetic induction cycler, MIC: user manual version 1.2. Brisbane: BMS. Available from: https://biomolecularsystems.com/mic-pcr [cited 24 Jun 2024]. |
| 13. | Ribeiro JC, Tamanini R, Soares BF, De Oliveira AM, De Godoi Silva F, Da Silva FF, et al. Efficiency of boiling and four other methods for genomic DNA extraction of deteriorating spore-forming bacteria from milk. Semina: Cienc Agrar 2016; 37(5): 3069–78. doi: 10.5433/1679-0359.2016v37n5p3069 |
| 14. | Thermo Fisher Scientific. NanoDrop™ Eight Spectrophotometer & Qubit™ Flex Fluorometer. 2024. Available from: https://www.thermofisher.com/order/catalog/product/NDE-QBFLEX [cited 29 June 2024]. |
| 15. | Lin WS, Cheng CM, Van KT. A quantitative PCR assay for rapid detection of Shigella species in fresh produce. Available from: http://frodo.wi.mit.edu/cgi-bin/primer3/primer3_www.cgi [cited 16 June 2024]. |
| 16. | Pavlovic M, Luze A, Konrad R, Berger A, Sing A, Busch U, et al. Development of a duplex real-time PCR for differentiation between E. coli and Shigella spp. J Appl Microbiol. 2011;110(5):1245–1. doi: 10.1111/j.1365-2672.2011.04973.x |
| 17. | BD PhoenixTM M50 System Quick Reference Guide PhoenixTM M50 System Quick Reference Guide. 2021. Available from: https://www.bd.com/resource.aspx?IDX=12345 [cited 5 August 2024]. |
| 18. | Clinical and Laboratory Standards Institute (CLSI). M100 performance standards for antimicrobial susceptibility testing. 33rd ed. Wayne, PA: CLSI; 2023. |
| 19. | Alemayehu A, Maru M, Bewket W, Assen M. Spatiotemporal variability and trends in rainfall and temperature in Alwero watershed, western Ethiopia. Environ Syst Res 2020; 9(1): 1–14. doi: 10.1186/s40068-020-00184-3 |
| 20. | World Health Organization. Improved sanitation facilities and drinking-water sources. Geneva: WHO. Available from: https://www.who.int/data/nutrition/nlis/info/improved-sanitation-facilities-and-drinking-water-sources [cited 19 November 2024]. |
| 21. | REDCap. The Ohio State University Center for Clinical and Translational Science grant support. REDCap (Research Electronic Data Capture). Available from: https://www.osu.edu [cited 16 August 2024]. |
| 22. | Carroll L. How to cite R and R packages. rOpenSci; 2021. Available from: https://ropensci.org/blog/2021/11/16/how-to-cite-r-and-r-packages/ [cited 3 June 2024]. |
| 23. | Girma M, Hussein A, Norris T, Genye T, Tessema M, Bossuyt A, et al. Progress in water, sanitation and hygiene (WASH) coverage and potential contribution to the decline in diarrhea and stunting in Ethiopia. Matern Child Nutr 2024; 20(S5): 1–13. doi: 10.1111/mcn.13280 |
| 24. | Sisay SF, Gari SR, Ambelu A. Water safety practices along the water service chain in Addis Ababa: a cross-sectional study in a Cosmopolitan City. Environ Health Insights 2024; 18: 1–9. doi: 10.1177/11786302241235006 |
| 25. | Ragupathi ND, Sethuvel DM, Inbanathan FY, Veeraraghavan B. Accurate differentiation of Escherichia coli and Shigella serogroups: challenges and strategies. New Microbes New Infect 2018; 21: 58–62. doi: 10.1016/j.nmni.2017.09.003 |
| 26. | Huruy K, Kassu A, Mulu A, Worku N, Fetene T, Gebretsadik S, et al. Intestinal parasitosis and shigellosis among diarrheal patients in Gondar teaching hospital, northwest Ethiopia. BMC Res Notes 2011; 4: 472. doi: 10.1186/1756-0500-4-472 |
| 27. | Federal Democratic Republic of Ethiopia. 2019. Available from: https://www.dhsprogram.com [cited 14 May 2025]. |
| 28. | Demissie TA. Prevalence and antimicrobial susceptibility patterns of Shigella and Salmonella species among patients with diarrhea attending Gondar Town Health Institutions, Northwest Ethiopia. Sci J Public Health 2014; 2(5): 469–74. doi: 10.11648/j.sjph.20140205.24 |
| 29. | Alemu A, Geta M, Taye S, Eshetie S, Engda T. Prevalence, associated risk factors and antimicrobial susceptibility patterns of Shigella infections among diarrheic pediatric population attending at Gondar town healthcare institutions, Northwest Ethiopia. Trop Dis Travel Med Vaccines 2019; 5(1): 1–7. doi: 10.1186/s40794-019-0079-7 |
| 30. | Mekonnen M, Geda B, Teklemariam Z, Weldegebreal F, Balakrishnan S. Prevalence of childhood diarrhea and associated risk factors in Dire Dawa, eastern Ethiopia. J Public Health (Germany) 2018; 26(1): 29–37. doi: 10.1007/s10389-017-0843-y |
| 31. | Muse K, Urgessa K, Shume T, Tahir B, Weldegebreal F. Prevalence, associated factors and antimicrobial susceptibility patterns of Salmonella and Shigella species among diarrheic under five children in Sultan Sheik Hassan Yabere referral Hospital, Jigjiga, Eastern Ethiopia. BMC Pediatr 2024; 24(1): 1–10. doi: 10.1186/s12887-024-04755-6 |
| 32. | Fana H, Mekonnen EH, Kebede A, Menkir S. Isolation rate and drug resistance patterns of Shigella species among diarrheal patients attending at. J Sci Technol. 2014; 7: 1–6. |
| 33. | Abate Chekol D, Gobena T, Mengiste B. Water supply accessibility and associated factors among households of Jigjiga Town, Eastern Ethiopia. Landscape Architect Region Plan. 2020; 5(1): 1. doi: 10.11648/j.larp.20200501.11 |
| 34. | Mama M, Alemu G. Prevalence, antimicrobial susceptibility patterns and associated risk factors of Shigella and Salmonella among food handlers in Arba Minch University, South Ethiopia. BMC Infect Dis 2016; 16(1): 1–8. doi: 10.1186/s12879-016-2035-8 |
| 35. | Marami D, Hailu K, Tolera M. Prevalence and antimicrobial susceptibility pattern of Salmonella and Shigella species among asymptomatic food handlers working in Haramaya University cafeterias, Eastern Ethiopia. BMC Res Notes 2018; 11(1): 1–6. doi: 10.1186/s13104-018-3189-9 |
| 36. | Centers for Disease Control and Prevention (CDC). Health Alert Network (HAN) health advisory: increasing prevalence of extensively drug-resistant Shigella. 2023. Available from: https://www.cdc.gov/han/2023/han00486.html [cited 3 June 2024]. |
| 37. | Centers for Disease Control and Prevention (CDC). Shigellosis – yellow book 2024. 2024. Available from: https://wwwnc.cdc.gov/travel/yellowbook/2024/infections-diseases/shigellosis [cited 3 June 2024]. |
| 38. | Salleh MZ, Nik Zuraina NMN, Hajissa K, Ilias MI, Banga Singh KK, Deris ZZ. Prevalence of multidrug-resistant and extended-spectrum beta-lactamase-producing Shigella species in Asia: a systematic review and meta-analysis. Antibiotics 2022; 11(11): 1–15. doi: 10.3390/antibiotics11111653 |
| 39. | Beyene AM, Gezachew M, Mengesha D, Yousef A, Gelaw B. Prevalence and drug resistance patterns of Gram-negative enteric bacterial pathogens from diarrheic patients in Ethiopia: a systematic review and meta-analysis. PLoS One 2022; 17(3): 1–26. doi: 10.1371/journal.pone.0265271 |
| 40. | Daly SW, Lowe J, Hornsby GM, Harris AR. Multiple water source use in low- and middle-income countries: a systematic review. J Water Health 2021; 19(3): 370–92. doi: 10.2166/wh.2021.205 |
| 41. | Berendes DM, Omore R, Prentice-Mott G, Fagerli K, Kim S, Nasrin D, et al. Exploring survey-based water, sanitation, and animal associations with enteric pathogen carriage: comparing results in a cohort of cases with moderate-to-severe diarrhea to those in controls in the vaccine impact on diarrhea in Africa (VIDA) study, 2015–2018. Clin Infect Dis 2023; 76(Suppl 1): 140–52. doi: 10.1093/cid/ciac918 |