ORIGINAL ARTICLE
Surveillance of healthcare-associated bloodstream infections in neonatal intensive care unit of a tertiary care hospital
Pue Rakshit1, Nitika Nagpal1, Tuhina Banerjee1* and Ashok Kumar2
1Department of Microbiology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India; 2Department of Paediatrics, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India
Abstract
Background and objective: Healthcare-associated infections (HAIs) are a serious threat to patient safety. They cause substantial morbidity and mortality across various healthcare settings, including neonatal intensive care units (NICUs). This study was undertaken to determine the incidence of HA bloodstream infection (HA-BSI) in the NICU of a tertiary care hospital.
Methodology: Data were collected in a systematic manner based on the Centers for Disease Control and Prevention (CDC) guidelines for the surveillance of HAI for a period of 1 year (Jan–Dec, 2022). The HAI rate was calculated using the following formula: No. of cases/No. of patient days × 1,000.
Result: Among the 1,085 admitted neonates, the incidence of HA-BSI was 15.80/1,000 patient days. HAI was seen in neonates having mean birth weight 1,722.5 ± 113.906 g, mean gestational age 29.6 ± 1.38, and mean duration of hospital stay 13.8 ± 4.081 days. Among the 80 cases of HA-BSI, recognized pathogens were 22 (27.5%) Klebsiella pneumoniae, 16 (20%) non-albicans Candida, 13 (16.25%) methicillin-sensitive Staphylococcus aureus, 10 (12.5%) Candida albicans, 10 (12.5%) Acinetobacter baumannii, 4 coagulase-negative staphylococci, 3 (3.75%) methicillin-resistant Staphylococcus aureus, 1 (1.25%) Escherichia coli, and 1 (1.25%) Enterococcus. The mortality rate was 56.78%.
Conclusion: The predominance of K. pneumoniae and A. baumannii as causative pathogens suggests the need of stringent infection control measures and targeted antimicrobial strategies to reduce the burden of HAI and improve patient outcomes.
Keywords: healthcare-associated infection; bloodstream; NICU; infection rate
Citation: Int J Infect Control 2026, 22: 23850 – http://dx.doi.org/10.3396/ijic.v22.23850
Copyright: © 2026 Pue Rakshit et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 5 May 2025; Revised: 16 July 2025; Accepted: 29 August 2025; Published: 20 April 2026
Competing interests and funding: NA.
*Tuhina Banerjee, Department of Microbiology, Institute of Medical Sciences, Varanasi 221005, Uttar Pradesh, India, Email: drtuhina105@bhu.ac.in, drtuhina@yahoo.com
Healthcare-associated infections (HAIs) pose a major threat to patient safety, thus causing significant morbidity and mortality globally (1). Standardized protocols of HAI surveillance across hospital networks can give significant data on the burden of HAI and also reveal gaps in implementation of infection control measures (2). To tackle these issues, it is crucial to develop and implement comprehensive hospital guidelines aimed at the prevention, monitoring, and management of HAIs within the Neonatal Intensive Care Unit (NICU). These guidelines are based on evidence-based practices and are specifically designed to meet the distinct physiological and clinical requirements of neonates. They offer a standardized framework for infection control practices, which encompass hand hygiene, antimicrobial stewardship, device care protocols, environmental disinfection, and staff training (3). We had previously studied several outbreaks of multidrug resistant organism (MDRO) in the neonatal unit of the tertiary care hospital (4–6). However, we could not implement any HAI surveillance during these outbreaks. More recently, we studied an outbreak of Non albicans Candida (NAC) in the same neonatal unit and analyzed the gaps with implementation of a standardized HAI surveillance program (6). The present study was performed to analyze the trends of healthcare-associated bloodstream infection (HA-BSI) in NICU through this initiated surveillance protocol.
Methods
Study site and details
This cohort study was conducted in the Department of Microbiology, and the 40-bedded NICU of the 2,200-bedded tertiary care hospital, Varanasi, India. This study consisted of data collected during 1-year period (Jan 2022–Dec 2022) and analyzed after collection.
Definitions
For the purpose of data collection, HAI was defined as infection with a date of event, > 2 calendar days after the hospital admission date. Date of event was considered as the date of first positive case occurs within the window period. HA-BSI was defined as a laboratory-confirmed HA-BSI. Recognized pathogens were defined as those enlisted as a cause of BSI in the Centers for Disease Control and Prevention (CDC) manual (7). An organism that commonly inhabits body surfaces as commensals was considered as contaminants as per the list of CDC manual.
Data collection
This study included the data of the neonates admitted in the NICU. An active patient (neonate)-based surveillance was done prospectively by the identification of the blood culture positive cases from the laboratory investigation records in the NICU. Data were collected by the Infection Prevention and Control (IPC) team consisting of microbiologists, pediatricians, and infection control nurses trained in HAI surveillance. Surveillance was performed by regular review of the microbiological data from the record files of the NICU through daily visits to the NICU. Data were collected based on the modules from European Centre for Disease Prevention and Control (ECDC), CDC (2), and National Healthcare Safety Network (NHSN) for surveillance purpose provided by national surveillance network. Along with microbiological data, clinical data based on features of physician’s suspicion of sepsis, in form of hypotension, hypothermia, respiratory distress, fever, apnea, and bradycardia were considered for selection of cases. Blood culture reports of probable contaminants were not considered.
Infection control practices
During this period, the IPC members monitor hand hygiene practices of the staff of NICU through direct observation. They also provided monthly feedbacks on compliance to hand hygiene followed with a review meeting with the staff of the NICU. At the same time, the staff were also repeatedly trained on surface cleaning and disinfection as per the hospital guidelines. Periodic environmental surveillance was done to detect the source of contaminants in the NICU environment.
Data analysis
The incidence of HA-BSI was calculated using the formula: No. of cases/No. of patient days × 1,000. To assess the effect of birthweight on the infection rate, all newborns were stratified to three categories: < 1,500 g, 1,500–2,500 g, and > 2,500 g.
Statistical analysis was performed by the two-way chi square test using MedCalc Statistical Software version 19.2.6 (MedCalc Software bv, Ostend, Belgium) to show the association of BSI with HAI and non-HAI neonates. Results with a P-value ≤ 0.05 were considered statistically significant.
Result
During the study period, 1,085 neonates were admitted in the NICU. The incidence of HA-BSI was 15.80/1,000 patient days. Neonates with birthweight < 1,500 g, 1,500–2,500 g, and > 2,500 g had HA-BSI incidence of 5.92, 6.12, and 3.75/1,000 patient days, respectively. The mean birth weight of neonates with HAI was 1,722.5 ± 113.90 (P = 0.0001), mean gestational age 29.6 ± 1.38 (P = 0.0148), and mean duration of hospital stay 13.8 ± 4.081. The mortality rate was 56.78%. The characteristics of the cases of HAI and non-HAI have been shown in Table 1. Mean birth weight of neonates and gestational age was significantly associated with HA-BSI.
| Characteristics | HAI (n = 76) N (%) | non-HAI (n = 295) N (%) | P |
| Mean gestational age (weeks) | 29.6 ± 1.38 | 30.13 ± 4.12 | 0.0148* |
| Mean birth weight (g) | 1,722.5 ± 113.90 | 2080.95 ± 673.67 | 0.0001* |
| Gender (male) | 47 (58.75) | 177 (60) | 0.7700 |
| Low birth weight (< 2,500 g) | 56 (59.90) | 218 (74) | 0.9698 |
| Mortality rate | 53 (66.25) | 178 (60.39) | 0.1323 |
| *P ≤ 0.05, significant. | |||
Of the total neonates, 371 (34.19%) were diagnosed as cases of neonatal sepsis, with a positive blood culture. The following pathogens were isolated: Klebsiella pneumoniae 21.02% (78/371), non-albicans Candida (NAC) 16.98% (63/371), Acinetobacter baumannii 13.47% (50/371), methicillin-sensitive Staphylococcus aureus 12.66% (47/371), Escherichia coli 9.70% (36/371), Candida albicans 7.54% (28/371), methicillin-resistant Staphylococcus aureus (MRSA) 6.73% (25/371), coagulase negative staphylococci (CoNS) 6.46% (24/371), and Enterococcus spp. 3.50% (13/371). However, as only a single blood culture was considered, CoNS was considered as contaminants. Of the 371 cases of neonatal sepsis, 76 cases were diagnosed as HA-BSI. Recognized pathogens in HA-BSI were 22 (27.5%) K. pneumoniae, 16 (20%) NAC, 13 (16.25%) S. aureus, 10 (12.5%) C. albicans, 10 (12.5%) A. baumannii, 3 (3.75%) MRSA 1 (1.25%) E. coli, and 1 (1.25%) Enterococcus. The distribution of organisms in HAI and non-HAI has been shown in Fig. 1, and the distribution of organisms according to birthweight of neonates has been shown in Fig. 2.
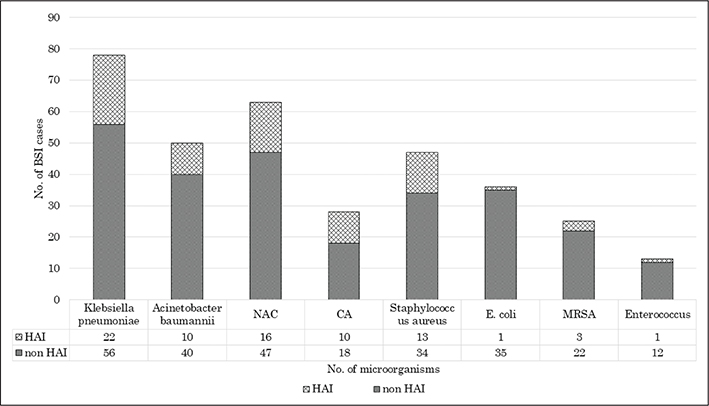
Fig. 1. Distribution of microorganisms causing bloodstream infections in the NICU, both HAI and non-HAI.
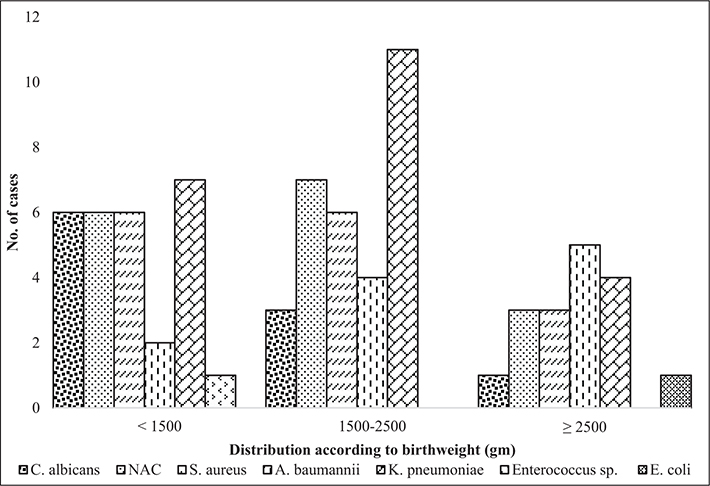
Fig. 2. Distribution of organisms associated with HA-BSI based on birth weight of the neonates (< 1,500 g, 1,500–2,500 g, and > 2,500 g).
Based on birth weight of the neonates, K. pneumoniae was the most common pathogen in neonates with < 1,500 g, 30.84% (28/76) and 1,500–2,500 g, 40.78% (31/76) groups, while A. baumannii was commonest in the > 2,500 g group, 22.36% (17/76).
For the organisms isolated from 76 HAI cases, susceptibility pattern for K. pneumoniae was for levofloxacin 71.42% (15/21), ciprofloxacin 61.90% (13/21), amikacin 70.58% (12/17), gentamicin 42.85% (9/21), meropenem 52.63% (10/19), imipenem 42.10% (8/19), while for A. baumannii, it was amikacin 72.72% (8/11), ciprofloxacin 63.63% (7/11), levofloxacin 45.45% (5/11), imipenem 54.54% (6/11), and meropenem 45.45% (5/11). All the Candida isolates were 100% (26/26) susceptible for fluconazole, itraconazole, and voriconazole. For S. aureus, susceptibility shown against vancomycin 100% (13/13) and linezolid 100% (13/13).
Among the total cases of neonatal sepsis, during the study period, the empirically used antibiotics were amikacin 61.45% (228/371), levofloxacin 43.93% (163/371), vancomycin 50.67% (188/371), fluconazole 28.03% (104/371), meropenem 22.10% (82/371), and piperacillin/tazobactam 6.73% (25/371).
Discussion
Over the past few decades, significant advances in NICU have led to remarkable improvements in the survival rates of neonates. These developments including better respiratory support, advance monitoring system, and refined nutritional support have undoubtedly contributed to saving countless lives and improving outcomes for these vulnerable populations.
Neonatal ICUs face alarmingly high rates of HA-BSIs particularly in low birthweight category, where rates reach 6.09/1,000 patient days (8). Neonates with a birthweight of < 1,500 g, 1,500–2,500 g, and > 2,500 g had HA-BSI incidence of 5.92, 6.12, and 3.75/1,000 patient days comparable to a multicentre study from India showing 21.00, 8.1, and 10.8/1,000 patient days, respectively, for the same birthweight categories in neonates (1). The overall incidence of HA-BSI was 15.80/1,000 patient days as compared with studies from India (13.2%) (9), Poland (7.32%) (10), and from Nepal (47%) (11). This can be due to poor maternal health, lack of skilled birth care, and weak healthcare access especially in rural areas. Neonates’ mortality remains a significant global health challenge; however, there is hope for further reductions in neonates’ mortality with continued progress in healthcare settings.
All the BSIs were primary, and none was associated with central line comparable to a study from India showing 74% BSIs were classified as primary BSI (1).
In the present study, K. pneumoniae was the most common pathogens associated with BSI in neonates, followed by A. baumannii and S. aureus, similar to a multicentre study from India, showing the same pattern of organisms that is K. pneumoniae (24.8%), A. baumannii (21.3%), and S. aureus (8.8%) (1). Another study from India showed that K. pneumoniae (39.39%) was the most common pathogen associated with HA-BSI (12), which is in line with studies from Italy showing K. pneumoniae as the most common pathogens, and the mortality rate of HA-BSI was higher with Gram-negative pathogens (36.4%) compared with Gram-positive (4.5%) (13). A study from South Korea showed that among the bacterial cases, S. aureus (65%) represented the majority cases of HA-BSI (14). Another study from Turkey showed that K. pneumoniae (25.9%) was the most common etiologic agents of HA-BSI (15), similar to that from Poland (29.3%) (10).
Klebsiella is a member of normal microbiota in the gastrointestinal and respiratory tracts. Additionally, hospital surfaces and high-touch equipment can act as reservoir for the bacteria. Another reason can be due to the immature immune system of the infants, which is less capable of defending against infections (16). A recent research on colonization of Carbapenem resistant Klebsiella pneumoniae (CRKP) on neonates has shown that CRKP can colonize skin and gut of neonates within 24–72 h of birth (17). Similarly, A. baumannii, which is also known for its high resistance to multiple antibiotics, can survive on surfaces and equipment for prolonged periods. The combination of its environmental persistence, resistance to treatments, and the high vulnerability of NICU patients contributes to A. baumannii, which is a common and challenging pathogen in intensive care units (18).
Although empirical use of antibiotics was high in this study, compared to another study from USA where over 95% of infants admitted to the NICU receive empirical antibiotics in the first postnatal days, only 1–5% have positive initial blood cultures (19). This can be due to difficulty in distinguishing between bacterial infection and non-infectious conditions in newborns, especially preterm infants with undeveloped immune systems. Clinicians may initiate antibiotics as a precautionary measure because early signs of infection can be nonspecific and potentially life threatening if left untreated. Additionally, delays in obtaining definitive culture results can lead to prolonged empirical antibiotic use. The lack of standard guidelines and fear of negative outcomes contribute further overuse of antibiotics in NICU settings (20).
This study has some limitations. A single blood culture criteria was used to diagnose BSI. Additionally, this study was conducted on a single NICU setting, which limits the generalizability of the findings to other healthcare facilities with differing infection control practices. Nevertheless, it reinstates the importance of HAI surveillance based on standardized protocols in order to intervene with adequate measures. The strength of this study was attributed to the systematic surveillance of HA-BSI in an extensive NICU cohort, and the correlation of low birth weight and gestational age with the risk of infection. This study provides valuable insights into the distribution of pathogens and their resistance patterns, thereby providing significant guidance for empirical treatment and infection management in neonatal care.
Conclusion
The increased occurrence of HA-BSI and the related mortality emphasize the urgent necessity for improved infection prevention measures in the NICU. The prevalence of multidrug-resistant organisms such as K. pneumoniae and A. baumannii underscores the significance of strong antimicrobial stewardship, prompt diagnosis, and focused treatment to reduce the effects of HAIs and enhance neonatal survival rates.
Acknowledgments
This research work was supported by staff under Grant No. M-22/0577 funded by Bill Melinda Gates Foundation. We would like to thank the staff of NICU for their cooperation in conducting the study.
Ethical approval
This study was approved by the Institute Ethical Committee via letter No. Dean/2021/EC/2598, dated: 10-04-2021.
References
| 1. | Mathur P, Malpiedi P, Walia K, Srikantiah P, Gupta S, Lohiya A, et al. Indian Healthcare Associated Infection Surveillance Network collaborators. Health-care-associated bloodstream and urinary tract infections in a network of hospitals in India: a multicentre, hospital-based, prospective surveillance study. Lancet Glob Health 2022; 10(9): 1317–25. doi: 10.1016/S2214-109X(22)00274-1 |
| 2. | IPC. Infection control guidelines and recommendations for healthcare settings. 2025. Available from: https://www.cdc.gov/infection-control/hcp/guidance/index.html [cited 5 April 2025]. |
| 3. | Mauger B, Marbella A, Pines E, Chopra R, Black ER, Aronson N. Implementing quality improvement strategies to reduce healthcare-associated infections: a systematic review. Am J Infect Control 2014; 42(10): 274–83. doi: 10.1016/j.ajic.2014.05.031 |
| 4. | Banerjee T, Bhattacharjee A, Upadhyay S, Mishra S, Tiwari K, Anupurba S, et al. Long-term outbreak of Klebsiella pneumoniae & third generation cephalosporin use in a neonatal intensive care unit in north India. Indian J Med Res 2016; 144(4): 622–9. doi: 10.4103/0971-5916.200900 |
| 5. | Sharma S, Das A, Garg R, Pramanik S, Marndi P, Singh R, et al. A reservoir of carbapenem-resistant Acinetobacter baumannii in the hospital environment and colonization pressure: a surveillance-based study in Indian intensive care unit. Microb Drug Resist 2022; 28(12): 1079–86. doi: 10.1089/mdr.2022.0088 |
| 6. | Banerjee T, Wangkheimayum J, Sharma S, Kumar A, Bhattacharjee A. Extensively Drug-resistant hypervirulent Klebsiella pneumoniae from a series of neonatal sepsis in a tertiary care hospital, India. Front Med (Lausanne). 2021; 8(8): 645955. doi: 10.3389/fmed.2021.645955 |
| 7. | CDC. Identifying healthcare-associated infections (HAI) for NHSN surveillance. Atlanta: Centers for Disease Control and Prevention; 2022. Available from: https://www.cdc.gov/nhsn/pdfs/pscmanual/2psc_identifyinghais_nhsncurrent.pdf [cited 3 April 2025]. |
| 8. | Johnson J, Malwade S, Agarkhedkar S, Randive B, Rajput UC, Valvi C, et al. Risk factors for health care-associated bloodstream infections in NICUs. JAMA Netw Open 2025; 8(3): 251821. doi: 10.1001/jamanetworkopen.2025.1821 |
| 9. | Kumar S, Shankar B, Arya S, Deb M, Chellani H. Healthcare associated infections in neonatal intensive care unit and its correlation with environmental surveillance. J Infect Public Health 2018; 11: 275–9. doi: 10.1016/j.jiph.2017.08.005 |
| 10. | Sadowska-Krawczenko I, Jankowska A, Kurylak A. Healthcare-associated infections in a neonatal intensive care unit. Arch Med Sci 2012; 8: 854–8. doi: 10.5114/aoms.2012.31412 |
| 11. | Yadav SK, Yadav SP, Bhatta NK, Kanodia P, Singh RR, Khanal B. Risk factors for hospital acquired bloodstream infections in neonatal intensive care unit of B.P. Koirala Institute of Health Sciences, Nepal. Sri Lanka J Child Health 2017; 46: 16–22. |
| 12. | Rakshit P, Nagpal N, Sharma S, Mishra K, Kumar A, Banerjee T. Effects of implementation of healthcare associated infection surveillance and interventional measures in the neonatal intensive care unit: small steps matter. Indian J Med Microbiol 2023; 44: 100369. doi: 10.1016/j.ijmmb.2023.100369 |
| 13. | Orsi GB, d’Ettorre G, Panero A, Chiarini F, Vullo V, Venditti M. Hospital-acquired infection surveillance in a neonatal intensive care unit. Am J Infect Control 2009; 37(3): 201–3. doi: 10.1016/j.ajic.2008.05.009 |
| 14. | Jeong IS, Jeong JS, Choi EO. Nosocomial infection in a newborn intensive care unit (NICU), South Korea. BMC Infect Dis 2006; 6: 103. doi: 10.1186/1471-2334-6-103 |
| 15. | Bolat F, Uslu S, Bolat G, Comert S, Can E, Bulbul A, et al. Healthcare-associated infections in a Neonatal Intensive Care Unit in Turkey. Indian Pediatr 2012; 49(12): 951–7. doi: 10.1007/s13312-012-0249-4 |
| 16. | Chang D, Sharma L, Dela Cruz CS, Zhang D. Clinical epidemiology, risk factors, and control strategies of Klebsiella pneumoniae infection. Front Microbiol 2021; 22(12): 750662. doi: 10.3389/fmicb.2021.750662 |
| 17. | Mishra K, Saini M, Pragya P, Sharma S, Rakshit P, Banerjee T, et al. High burden of Carbapenem-resistant Klebsiella pneumoniae (CRKP) colonization in neonates in a tertiary care hospital in India. J Pure Appl Microbiol 2025; 19(1): 227–34. doi: 10.22207/JPAM.19.1.13 |
| 18. | Peleg AY, Seifert H, Paterson DL. Acinetobacter baumannii: emergence of a successful pathogen. Clin Microbiol Rev 2008; 21(3): 538–82. doi: 10.1128/CMR.00058-07 |
| 19. | Anstey NM, Currie BJ, Hassell M, Palmer D, Dwyer B, Seifert H. Community-acquired bacteremic Acinetobacter pneumonia in tropical Australia is caused by diverse strains of Acinetobacter baumannii, with carriage in the throat in at-risk groups. J Clin Microbiol 2002; 40(2): 685–6. doi: 10.1128/JCM.40.2.685-686. |
| 20. | Camacho-Gonzalez A, Spearman PW, Stoll BJ. Neonatal infectious diseases: evaluation of neonatal sepsis. Pediatr Clin North Am 2013; 60(2): 367–89. doi: 10.1016/j.pcl.2012.12.003. |