SHORT REPORT
Cross-infection risk related to use of portable fans in a healthcare setting
Chloe Hylton*, Kerryanne Brown and Kalani Mortimer
Microbiology Department, Mersey and West Lancashire Teaching Hospital NHS Trust, Prescot, United Kingdom
Abstract
Hospital environments pose infection risks. During a meticillin resistant Staphylococcus aureus (MRSA) outbreak in an adult Intensive Care Unit (ICU), a visibly contaminated bladeless Dyson® fan at the bedside of a previous outbreak patient prompted a microbiological investigation. Four sections of the bladeless Dyson® fan were swabbed to identify potentially pathogenic organisms, with confirmed isolates undergoing whole genome sequencing. Results identified MRSA, vancomycin resistant Enterococcus (VRE) and Aspergillus niger. The MRSA strain identified on the bladeless fan matched the outbreak strain.
Existing research acknowledges the infection risks associated with inadequate ventilation and the use of fans in healthcare settings. The pandemic highlighted the importance of ventilation; however, comprehensive guidance on the use of portable fans in healthcare settings is yet to be provided. The contaminated fan was removed and disposed of, and trust wide communication was given recommending all portable fans to be removed from the trust.
This case study confirmed the presence of potential pathogens on a bladeless Dyson® fan in an ICU. This further highlights the need for cleanable fan designs and research into the safe use of these devices to mitigate infection risks whilst addressing ventilation and cooling needs in healthcare settings.
Keywords: IPC; Fans; MRSA; NHS; cross-infection hazard
Citation: Int J Infect Control 2026, 22: 23842 – http://dx.doi.org/10.3396/ijic.v22.23842
Copyright: © 2025 Chloe Hylton et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 4 April 2025; Revised: 29 July 2025; Accepted: 5 August 2025; Published: 28 April 2026
Competing interests and funding: The authors declare there is no conflict of interest. No funding was received. Outbreak investigation was done as part of a clinical/infection control practice and resources were used as part of routine available resource.
*Chloe Hylton, Microbiology Department, Mersey and West Lancashire Teaching Hospital NHS Trust, Prescot, United Kingdom. Email: Chloe.hylton@merseywestlancs.nhs.uk
Patients and staff are at risk of acquiring infection from the hospital environment, especially in insufficiently ventilated spaces (1). Inadequate ventilation and/or temperature control can lead to the use of portable, domestic fans in healthcare settings to maintain patient and staff comfort. However, use of such fans may create a cross-infection hazard.
An environmental review was conducted during the outbreak of meticillin-resistant Staphylococcus aureus (MRSA) on a general adult Intensive Care Unit (ICU) which identified a visibly contaminated bladeless Dyson® fan (Dyson Ltd, Wiltshire, UK) as shown in Fig. 1, in a side room located at the bedside which previously occupied an outbreak patient. It was not possible to determine how or if this fan was cleaned previously. This prompted microbiological investigation of the contaminated fan to assess if potentially pathogenic organisms were present.
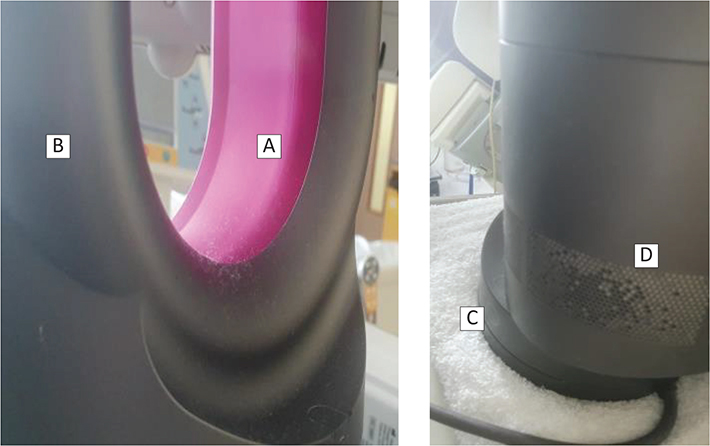
Figure 1. The visibly contaminated bladeless Dyson® fan, unable to be adequately cleaned (especially the air inlet grid). (A) inner casing, (B) outer casing, (C) swivel base, (D) air inlets.
Materials and methods
Four areas of the fan were sampled using PolywipeTM swabs (Medical Wire and Equipment Co Ltd, Wiltshire, UK): inner casing, outer case, swivel base and air inlets (Figure 1). The swabs were placed into brain heart infusion (BHI) broths (E & O Laboratories, Bonnybridge, UK) and incubated in air at 37°C. A single negative control was set up during each day of sampling by placing an unused PolywipeTM swab into the BHI broth.
After 24-h of incubation, a 10 µL sample from each broth was inoculated on to ColorexTM MRSA chromogenic media, ColorexTM Vancomycin resistant Enterococcus (VRE) Chromogenic media, ColorexTM mSuperCARBATM Carbapenamase producing Enterobacterales (CPE) chromogenic agar and Sabouraud (SAB) Dextrose Agar with Chloramphenicol selective media (all media from E & O laboratories, Bonnybridge, UK) for the identification of fungi. The media were incubated for 24-h in air at 37°C and reviewed daily for 5 days. The SAB culture was incubated at 37°C for 48 h and then incubated at 30°C for a further 8 days. Confirmed isolates were referred to United Kingdom Health Security Agency (UKHSA) Colindale for whole genome sequencing.
Results
After 24 h of incubation, three out of four sites of the fan (inner casing, outer casings and swivel base) were positive for MRSA. VRE, CPE and fungal cultures were negative. On day 6 the air inlet grid was culture positive for MRSA, VRE and Aspergillus niger. All other sites were negative on further incubation as shown in Table 1.
| Day 0 | Day 1 | Day 2* | Day 3 | Day 4 | Day 5 | Day 6 | Day 7–10 | |
| Inner Casing | Subculture onto MRSA, VRE, CPE and SAB | MRSA identified | No growth | No growth | No growth | No growth | No growth | No further fungal growth |
| Outer Casing | Subculture onto MRSA, VRE, CPE and SAB | MRSA identified | No growth | No growth | No growth | No growth | No growth | No further fungal growth |
| Swivel Base | Subculture onto MRSA, VRE, CPE and SAB | MRSA identified | No growth | No growth | No growth | No growth | No growth | No further fungal growth |
| Air Inlet | Subculture onto MRSA, VRE, CPE and SAB | No growth | No growth | No growth | No growth | No growth | MRSA identified, VRE identified and Aspergillus niger identified via the SAB plate | No further fungal growth |
| Negative control | No growth | No growth | No growth | No growth | No growth | No growth | No growth | No further fungal growth |
| *SAB culture was moved to 30°C after 48 h of no growth for fungi. | ||||||||
The MRSA isolated from the fan was confirmed as identical to the outbreak strain by whole genome sequencing conducted by the Antimicrobial Resistance and Healthcare Associated Infections Laboratory, UKHSA.
Discussion
A growing body of literature has examined the impact of fans, ventilation systems and other environmental factors on infection control and patient safety within healthcare settings (2). Wong et al. (3) described the use of indoor fans facilitating air dispersal of MRSA in residential care homes. Brooks et al. (4) highlight the practical challenges relating to heatwaves in a healthcare setting. Lenzer et al. (5) describe the potential benefits to patients’ health and to wider healthcare systems of heating, ventilation, air conditioning (HVAC) and fans. Dhanda et al. (6) and Alsaffar et al. (7) discuss bacterial colonisation and cross-infection risks associated with bladeless fans and highlight the potential dangers posed by these devices in healthcare environments.
There is a lack of comprehensive guidelines or consensus regarding the safe use of fans in healthcare settings with a lack of device cleaning instructions. Documents such as the Estates and Facilities Alert (8) and guidelines by Health Protection Scotland (9) caution against the potential infection risks associated with fans, but do not provide detailed protocols or mitigation strategies.
There has been an increased focus on ventilation in healthcare facilities since the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic. During the pandemic, we recommended against the use of fans in clinical areas; however, post-pandemic the use of fans began to creep in. In a considerable proportion of the NHS estate, there is insufficient ventilation to keep patients and staff comfortable (which is becoming an increasing phenomenon, attributable to climate change) (4). Development of fans which are cleanable and minimise trapping of dust and debris, that can be used safely in a healthcare setting, would be useful to maintain patient and staff comfort in settings with sub-optimal ventilation/temperature control more safely.
Whilst it is not possible to determine whether the fan was the source of this outbreak, this case provides an insight into the risks associated with colonisation of fans with potential pathogens and their potential to contribute to cross-transmission. Routine environmental swab sampling is not performed within our trust unless required in exceptional circumstances such as outbreaks which continue despite implementation of standard control measures; in this case, the fan was swabbed due to being grossly visibly contaminated, no attempt was made to clean the device. Although it would be possible to surface disinfect the inner casing (A) and the out casing (B) of the fan as shown in figure 1, it is not possible clean the air inlet grids effectively without dismantling the device. Neither the manufacturer of Dyson® fan bladeless nor bladed fans provide instructions on how they can be adequately cleaned. As it is not possible to clean the bladeless fan’s air inlet grids without dismantling the device, the advice from our Trust’s Medical Device Management Team was that it is not acceptable from an electrical safety point of view to dismantle the fan for cleaning in the absence of specific instructions by the manufacturer. Trust-wide communication was issued by the Ventilation Safety Group (VSG) informing of the inability of bladeless fans to be cleaned effectively, the risk of them becoming contaminated with hazardous organisms, followed by the recommendation that fans in clinical areas should be removed.
In areas of the trust where there is adequate temperature control via the building management system, staff were informed to keep the door/windows closed so that the system can maintain temperature as per design; in any areas where the temperature provided by the building management system was too high, users of those areas were advised to liaise with the Estates and Facilities team to have the temperature lowered to acceptable levels. Figure 2 provides additional guidance issued to staff regarding keeping cool in hot weather.

Figure 2. Communication of hot weather alert, providing additional guidance for keeping cool (10).
In clinical areas of the trust where there is no temperature control, the VSG suggested conventional fans to be supplied by the Estates and Facilities team during exceptional circumstances such as heatwaves, as these are easier to clean/disinfect as they lack air inlet grids in contrast to the Dyson bladeless fans; thus, they can be surface disinfected with an appropriate agent such as 1,000 parts per million chlorine, or equivalent, without the need to dismantle the device thus potentially compromising its electrical safety.
The bladed fans would be disinfected between patients by ward staff. When the period of hot weather ends, the fans would be removed, cleaned and stored away from clinical areas by the Estates and Facilities Team. Whilst this is not ideal, it was felt to be better than the option of clinical areas procuring/storing their own fans which are less likely to get cleaned adequately.
Conclusion
We demonstrated the presence of several potentially pathogenic organisms (including an outbreak strain of MRSA) from a bladeless Dyson® fan used on an ICU. Whilst it is not possible to determine whether the contamination identified on the fan contributed to the outbreak, this case study demonstrates the difficulty in the cleaning of the bladeless fans and the need for comprehensive guidance on how to safely use them. Whilst existing studies explore infection risks linked to fans, there is a lack of comprehensive guidelines on their safe use. Further research is needed to establish clear mitigation strategies for minimising infection risks associated with portable fans whilst balancing ventilation and cooling needs in healthcare settings.
Acknowledgements
The authors thank Oonagh McGugan for her support in conducting the environmental sampling.
Ethical statement
Informed consent was not obtained from patients involved in this outbreak. All patients were treated according to clinical judgment and infection control practices to treat them and control the outbreak according to local guidelines. Patients did not undergo randomization or intervention for the purpose of this report. Data has been analysed and presented anonymously.
Credit author statement
Chloe Hylton: Investigation, writing-original draft, writing-review and editing.
Kerryanne Brown: writing-original draft, writing-review and editing.
Dr. Kalani Mortimer: Conceptualisation, investigation, supervisor, writing-review and editing.
References
| 1. | Li H, Cui Q, Kong X, Fan M. Study on the infection control performance under interactive cascade ventilation: a focus on a conference room environment. Build Environ 2024; 250: 111161. doi: 10.1016/j.buildenv.2024.111161 |
| 2. | Body R. Do fans spread infection in clinical areas? Emerg Med J 2008; 25(10): 689. doi: 10.1136/emj.2008.065706 |
| 3. | Wong WC, Chen JH-K, Yuen LL-H, Chan VW-M, AuYeung CH-Y, Leung SS-M, et al. Air dispersal of meticillin-resistant Staphylococcus aureus in residential care home for the elderly: implications for transmission during the COVID-19 pandemic. J Hosp Infect. 2022; 123: 52–60. doi: 10.1016/j.jhin.2022.02.012 |
| 4. | Brooks K, Landeg O, Kovats S, Sewell M, O’Connell E. Heatwaves, hospitals, and health system resilience in England: a qualitative assessment of frontline perspectives from the hot summer of 2019. BMJ Open 2023; 13(3): e068298. doi: 10.1136/bmjopen-2022-068298 |
| 5. | Lenzer B, Rupprecht M, Hoffmann C, Hoffmann P, Liebers U. Health effects of heating, ventilation, and air conditioning on hospital patients: a scoping review. BMC Public Health 2020; 20(1): 1287. doi: 10.1186/s12889-020-09358-1 |
| 6. | Dhanda J, Gray J, White H. Bacterial cross-infection related to the use of bladeless fans in a clinical setting. J Hosp Infect. 2019; 103(4): 478–80. doi: 10.1016/j.jhin.2019.08.020 |
| 7. | Alsaffar L, Osborne L, Bourne NT. Bacterial colonization of bladeless electrical fans. J Hosp Infect. 2018; 100(4): 476–77. doi: 10.1016/j.jhin.2018.08.020 |
| 8. | Estates and Facilities Alert. Portable fans in health and social care facilities: risk of cross infection. Reference: EFA/2019/00. Crown Publication. London: NHS England; 2019. |
| 9. | Health Protection Scotland. SBAR: Portable cooling fans for use in clinical areas. 2018. Available from: https://www.nipcm.hps.scot.nhs.uk/media/1659/2018-08-sbar-fans-v1.pdf [cited 21 June 2025]. |
| 10. | NHS England. Hot weather alert: tips for staff and patients. [infographic]. Internal communication. Prescot: Mersey and West Lancashire Teaching Hospitals; 2024. |