ORIGINAL ARTICLE
Unveiling trends – healthcare-associated infections and prevention strategies in a tertiary care teaching hospital: a 5-year prospective surveillance study
Bashir Fomda1*, Uksim Qadri1, Gulnaz Bashir1, Akbar Shah2, Sehrish Baqal1, Abdul Waheed Mir2, Shaista Nazir1, Saleem Javaid Wani3 and Munaza Aman1
1Department of Microbiology, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, India; 2Department of Critical Care, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, India; 3Department of General Medicine, Sher-i-Kashmir Institute of Medical Sciences, Srinagar, India
Abstract
Background: Healthcare-associated infections (HAIs) pose a major threat to critically ill intensive care unit (ICU) patients. Limited data on HAIs in Indian ICUs necessitated this study at a tertiary care hospital in North India.
Objective: To determine the incidence, distribution, and causative agents of HAIs, assess their antibiotic susceptibility profile, and evaluate the impact of infection prevention and control (IPC) measures.
Design: This prospective study was conducted in the ICU settings of a tertiary care centre. Bloodstream infections (BSIs), central line-associated bloodstream infections (CLABSIs), urinary tract infections (UTIs), and catheter-associated urinary tract infections (CAUTIs) were defined according to standard definitions. The incidence and device utilisation ratio (DUR) were calculated. Identification and susceptibility were determined via BacT Alert and VITEK-2 Compact System. IPC compliance, including hand hygiene and central line insertion practices (CLIP), was monitored as per checklist.
Results: Overall BSI rates of 12.85 per 1,000 patient-days, CLABSI at 22.11 per 1,000 central line-days, and CAUTI at 1.77 per 1,000 urinary catheter-days were recorded. The DUR was calculated to be 0.44 and 0.6 for CLABSI and CAUTI respectively. Burkholderia cepacia (52.8%) was the predominant CLABSI pathogen, while Acinetobacter spp. (22.2%) was the most common CAUTI pathogen. Hand hygiene compliance improved from 40% in 2019 to 70% in 2023, CLIP adherence increased from 30 to 75%, CLABSI and CAUTI rate reduced from 19.66 to 8.59 and 8.66 to 0.75, respectively.
Conclusion: The study highlights the need for stringent IPC measures, robust antibiotic stewardship, and continuous surveillance to mitigate HAIs.
Keywords: Healthcare-associated infections; CLABSI; CAUTI; infection prevention and control; hand hygiene compliance
Citation: Int J Infect Control 2026, 22: 23839 – http://dx.doi.org/10.3396/ijic.v22.23839
Copyright: © 2026 2026 Bashir Fomda et al. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 22 March 2025; Accepted: 21 November 2025; Published: 29 June 2026
Competing interests and funding: The authors have no relevant financial or non-financial interests to disclose. The U.S. Centers for Disease Control and Prevention provided financial support for this research under Grant I.D. 53/CDC/TC/2017.
*Olufunmilola Makanjuola, Professor and Head, Department of Microbiology., Sher-i-Kashmir Institute of Medical Sciences, Soura, Srinagar, Jammu and Kashmir, India., Tel.: +919419001701. Email: bashirfomda@gmail.com
Healthcare-associated infections (HAIs), also known as nosocomial or hospital infections, are infections acquired by patients during their stay in a hospital or healthcare facility that were not present or incubating at the time of admission. Typically, HAIs manifest 48–72 h after hospitalization but can also develop post-discharge, usually within 10 days. They include infections acquired by healthcare staff and those transmitted to neonates during delivery (1, 2). HAIs remain a major concern for critically ill patients in intensive care units (ICUs), where their incidence is notably higher compared to general wards due to the patients’ heightened vulnerability and the frequent use of invasive procedures (3). The overall prevalence of HAIs worldwide varies from 5 to 10% across different healthcare settings (4). In the United States, HAIs are among the top 10 leading causes of death (5, 6). According to the WHO, approximately 7 out of every 100 patients in acute-care hospitals in high-income countries (HICs) and 15 out of every 100 patients in low- and middle-income countries (LMICs) acquire at least one HAI during their hospital stay, with a 10% mortality rate among those affected (1). HAIs contribute to increased morbidity and mortality, extended hospital stays, excessive antibiotic use, the risk of multidrug-resistant (MDR) pathogens, and higher healthcare costs. The most critical HAIs include central line-associated bloodstream infections (CLABSI), catheter-associated urinary tract infections (CAUTI), skin and soft tissue infections (SSTI), surgical site infections (SSI), ventilator-associated pneumonia (VAP), hospital-acquired pneumonia (HAP), and Clostridioides difficile colitis (CDI), with bacteria responsible for approximately 90% of these infections (7). Excessive antibiotic use has led to the emergence of MDR bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant Enterococcus faecium (VRE), carbapenem-resistant Pseudomonas aeruginosa, and extended-spectrum cephalosporin-resistant Klebsiella pneumoniae, which are significant complications of HAIs (8, 9). These resistant strains limit treatment options, complicate medical management, and prolong hospitalizations. In recent decades, hospitals have increasingly focused on combating HAIs. Many institutions have implemented comprehensive infection tracking and surveillance systems, alongside robust prevention strategies aimed at reducing infection rates (10).
Background
The prevention of HAIs is a collective responsibility of healthcare institutions and their staff, requiring collaborative efforts to minimise infection risks for both patients and personnel. Surveillance of HAIs is a crucial component of infection control and is recognized globally as a fundamental preventive measure. Local surveillance data are vital for guiding empirical treatment and ensuring effective therapy. However, data on HAI epidemiology in ICUs in India remains limited. In order to address this gap, we conducted a 5-year surveillance study (2018–2023) in the ICUs of a tertiary care teaching hospital in North India. To the best of our knowledge this is the largest single-center study from our region on this issue. The primary objective of this study was to determine the incidence, distribution, and causative agents of HAIs and their antibiotic susceptibility patterns. The secondary objective was to assess the impact of enhanced infection prevention and control (IPC) practices on the reduction of HAI rates.
Methods
Study design
This is a prospective surveillance study conducted from 2018 to 2023, in a 1,050-bedded super-speciality tertiary care hospital. It has 52 ICU beds distributed across medical, surgical, pediatric, neonatal, and critical-care units, all offering 24-h invasive, monitoring and ventilatory support. This study was a part of multicentric project entitled ‘Capacity Building and Strengthening of Hospital Infection Control to detect and prevent antimicrobial resistance in India’, funded by the Centers for disease control and prevention (CDC) and coordinated by All India Institute of Medical Sciences (AIIMS), New Delhi. The surveillance program initially prioritised bloodstream and urinary tract device-associated infections. HAP and VAP were not included in this study.
Implementation
A dedicated surveillance team worked in close coordination with clinical and laboratory staff to identify positive cultures relevant to HAIs under surveillance. For each positive blood or urine culture, additional clinical information was collected to confirm whether the case met the standardized HAI definitions. ICU personnel, trained in case definitions, actively assisted in identifying potential cases and notifying the surveillance team for verification.
The surveillance teams monitored infection rates, isolated pathogens, and antimicrobial susceptibility patterns in ICUs while also overseeing adherence to infection prevention measures, including hand hygiene and central line insertion practices (CLIP). The hand-hygiene program followed WHO multimodal strategies, incorporating the use of 70% isopropanol-based hand rubs, staff training, visual reminders, and checklist-based documentation. The central line insertion bundle included maximal sterile barrier precautions, 2% chlorhexidine skin antisepsis, daily review of line necessity, and checklist-based documentation using the CLIP tool. Compliance was monitored monthly and performance feedback was provided to ICU teams.
Patient logs were meticulously maintained, recording admission and discharge dates, transfers, laboratory results, and clinical documentation. Data collection was conducted by trained infection control nurses under the direct supervision of the principal and co-investigators. Surveillance data were gathered using standardized checklists and analyzed to determine the incidence of bloodstream infections (BSI), CLABSI, non-CLABSI, secondary CLABSI, and CAUTIs.
Regular capacity-building was ensured through onsite workshops and virtual ECHO (Extension for Community Healthcare Outcomes) sessions. The central coordinating team conducted routine site visits to ensure data quality, using standardized assessment tools to identify gaps and inaccuracies, followed by structured feedback. Refresher training sessions were also organized biannually during network investigator meetings to reinforce standardized surveillance methods.
Stringent validation measures were implemented to identify and reject erroneous entries from the Healthcare-Associated Infections Surveillance (HAIS) database. The nodal officer verified and approved data before submission, and the central team conducted monthly reviews to detect inconsistencies and address deficiencies.
Case definitions
Healthcare-Associated Infection (HAI): Defined as an infection that develops 48 h or more after ICU admission, diagnosed according to the Diagnostic Criteria for Nosocomial Infections by the CDC.
Primary BSI: A BSI without a matching positive culture from another body site within 14 days before or 7 days after the event date.
CLABSI: A primary BSI in a patient with a central line in place for more than 2 calendar days on the event date or in a patient whose central line was removed on the event date or the day before.
Secondary BSI: A BSI with a matching positive culture from another body site within 14 days before or 7 days after the event date.
Culture-Confirmed Urinary Tract Infection: A positive urine culture showing no more than two species of organisms or at least one organism with ≥ 105 colony-forming units/ml in a symptomatic patient (symptoms such as fever > 38°C, suprapubic tenderness, urgency, frequency, dysuria).
CAUTI: A culture-confirmed urinary tract infection (UTI) in a patient with an indwelling catheter in place for more than 2 calendar days on the event date or in a patient whose catheter was removed on the event date or the day before.
Data Calculation: Device-associated HAI rates were calculated using the following formulas:
- CLABSI Rate:

- CAUTI Rate:

- Device Utilization Ratio:
- Device days refer to the total days of exposure to each device (central venous line or urinary catheter) for all patients during the study period. Patient days denote the total number of days patients spent in the ICU during the selected period.
Case finding
Pathogens causing BSIs were reported as CLABSI if isolated from blood cultures of symptomatic patients meeting case definition criteria. Commensals isolated on the same or consecutive days from two matching blood cultures were also classified as CLABSI. A single organism with ≥ 105 CFU/mL isolated from the urine of a symptomatic patient meeting case definition criteria was classified as CAUTI. Case details were documented in reporting forms. Identification and antibiotic susceptibility tests were performed using the BacT Alert and VITEK Compact System. Compliance with hand hygiene and CLIP was monitored using checklists. Surveillance staff recorded hand hygiene moments attempted by healthcare providers, calculating compliance percentage by dividing the number of attempts by total opportunities. Compliance with CLIP was assessed as per CLIP tools. Patients were monitored until discharge from the ICU or death. Clinical details, antibiotic prescriptions, and device insertion dates and sites were recorded. Checklists for care bundles were used alongside clinical and hospital monitoring data, including patient demographics, admission and discharge dates, device use, pathogen isolation, and susceptibility patterns.
Data analysis
Numerator and denominator data were entered into the indigenously developed HAI surveillance database (www.haisindia.com). Patient confidentiality was maintained by removing all personal identifiers and assigning a unique identification number to each record. The software automatically compiled and analysed the data to generate monthly HAI rates and device utilisation ratios (DUR). Cumulative HAI and DUR data for all ICUs were obtained from the portal for the 5-year study period.
Statistical analysis
Data were entered and analyzed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables, including time to infection and total length of hospital stay, were summarized as mean (in days) ± standard deviation (SD). The Shapiro–Wilk test was applied to assess the normality of distribution for continuous variables. Depending on data distribution, comparisons between two groups were made using the independent samples t-test or the Mann–Whitney U test, while comparisons across more than two groups were performed using one-way analysis of variance (ANOVA) or the Kruskal–Wallis test. Categorical variables, such as gender, age group, and clinical outcome, were presented as frequencies and percentages, and associations between categorical variables were assessed using the Chi-square test or Fisher’s exact test when appropriate. A P-value < 0.05 was considered statistically significant.
Results
From 2018 to 2023, our institution recorded a total of 68,662 patient-days, 29,984 central line-days, and 41,191 urinary catheter-days. During this period, 735 HAIs were documented. Out of these, a total of 663 were CLABSI events, 438 (66.0%) occurring in males and 225 (34.0%) in females. The median age of patients developing CLABSI was 46 years (range 1–89 years), with the majority belonging to the 19–64 year age group (62.4%).
The overall median time to infection was approximately 10 days (Interquartile range/IQR 5–18 days) following ICU admission, while the median total length of stay (LOS) was 23 days (IQR 14–34 days). Gender differences were not statistically significant for either time to infection or LOS (P > 0.05). Patients who remained in the surveillance unit or were discharged exhibited longer LOS (mean > 30 days), whereas those who died or were transferred had substantially shorter LOS (P < 0.0001). Similarly, age had a moderate effect on both metrics, with older adults (≥ 65 years) showing slightly longer LOS than younger patients.
Among 72 CAUTI events, males and females were equally affected (36 each; 50.0%). The median age was 54 years (range 1–86 years), with 76.4% of cases occurring in adults aged 19–64 years. The median time to infection after ICU admission was 9 days (IQR 4–15 days), and the median total LOS was 22 days (IQR 13–33 days). No statistically significant gender difference was observed in either parameter (P > 0.05). Patients aged ≥ 65 years demonstrated longer LOS compared with younger groups. The 14-day outcome analysis revealed that 58.3% of patients had died within 2 weeks of infection, while 9.7% remained in the surveillance unit. Tables 1 and 2 show the 14-day and final outcomes of CLABSI and CAUTI patients.
| Parameters | CLABSI events (N = 663) | Time to infection (mean; in days) | P-value | Total length of stay (mean; in days) | P-value | ||
| Gender | |||||||
| Female | 225 (34.0) | 10.9 | P = 0.484 | 21.1 | P = 0.292 | ||
| Male | 438 (66.0) | 15.2 | 25.6 | ||||
| Age (years) | |||||||
| ≤ 18 | 192 (29.0) | 8.8 | P = 0.660 | 20.7 | P = 0.724 | ||
| 19–64 | 413 (62.4) | 16.6 | 25.7 | ||||
| ≥ 65 | 58 (8.7) | 10.2 | 23.7 | ||||
| 14 day outcome | |||||||
| Died | 271 (40.9) | 8.5 | P = 0.406 | 10.8 | P < 0.0001# | ||
| Transferred to other ward/unit within the hospital | 127 (19.2) | 29.3 | 38.8 | ||||
| Discharged | 73 (11.0) | 6.4 | 11.4 | ||||
| Transferred to other hospital | 2 (0.2) | 23.0 | 28.5 | ||||
| Still in surveillance unit | 190 (28.7) | 13.5 | 38.1 | ||||
| Final outcome | |||||||
| Died | 360 (54.3) | 9.6 | P = 0.525 | 16.7 | P = 0.013# | ||
| Transferred to other hospital | 4 (0.5) | 13.2 | 22.5 | ||||
| Discharged | 299 (45.2) | 18.7 | 33.0 | ||||
| CLABSI: central line-associated bloodstream infections; #: Statistically significant (P < 0.05). | |||||||
| Parameters | CAUTI events (N = 72) | Time to infection (mean; in days) | P-value | Total length of stay (mean; in days) | P-value | ||
| Gender | |||||||
| Male | 36 (50.0) | 13.9 | P = 0.770 | 27.6 | P = 0.494 | ||
| Female | 36 (50.0) | 13.2 | 23.9 | ||||
| Age (years) | |||||||
| ≤ 18 | 11 (15.3) | 11.8 | P = 0.736 | 38.3 | P = 0.131 | ||
| 19–64 | 55 (76.4) | 14.1 | 23.2 | ||||
| ≥ 65 | 6 (8.3) | 11.7 | 26.3 | ||||
| 14 day outcome | |||||||
| Died | 42 (58.3) | 13.3 | P = 0.466 | 14.4 | P < 0.0001# | ||
| Transferred to other ward/unit within the hospital | 21 (29.2) | 14.3 | 38.9 | ||||
| Still in surveillance unit | 7 (9.7) | 16.0 | 59.7 | ||||
| Discharged | 2 (2.8) | 2.5 | 7.5 | ||||
| Final outcome | |||||||
| Died | 46 (63.9) | 13.8 | P = 0.876 | 17.2 | P < 0.0001# | ||
| Transferred to other hospital | 1 (1.4) | 9.0 | 17.0 | ||||
| Discharged | 25 (34.7) | 13.4 | 41.9 | ||||
| CAUTI: catheter-associated urinary tract infections; #: Statistically significant (P < 0.05). | |||||||
The total BSI rate was 12.85 per 1,000 patient-days, with a CLABSI rate of 22.11 per 1,000 central line-days, a UTI rate of 1.06 per 1,000 patient-days, and a CAUTI rate of 1.77 per 1,000 urinary catheter-days. The DUR were 0.44 for CLABSI and 0.6 for CAUTI. Tables 1 and 2 provide the annual distribution of HAIs and DUR over the past 5 years. During these 5 years, adherence to hand hygiene improved, and CLIP increased from 40% in 2019 to 70% currently. Furthermore, adherence to central line insertion protocols rose from 30% in 2019 to 75% in 2023. The CLABSI rate at our hospital decreased from 19.66 to 8.59 per 1,000 central line-days, while the CAUTI rate fell from 8.66 to 0.75 per 1,000 urinary catheter-days (Tables 3 and 4). The overall mortality rate of 58.3% was observed among these patients.
A statistically significant downward trend was observed in device-associated infection rates across the 5-year surveillance period. The incidence of CLABSI showed a consistent reduction from 30.74 per 1,000 central line-days in 2018 to 11.44 per 1,000 central line-days in 2023 (χ2<sub>trend</sub> = 9.87, P = 0.002), indicating sustained improvement in central line care practices. Similarly, CAUTI rates declined markedly from 8.66 per 1,000 catheter-days in 2018 to 0.75 per 1,000 catheter-days in 2023 (χ2<sub>trend</sub> = 11.24, P = 0.001).
Microbial etiology of HAIs: The predominant organism isolated from CLABSI was Burkholderia cepacia (n = 438, 52.8%), followed by K. pneumoniae (n = 136, 16.4%), Acinetobacter spp. (n = 128,15.4%), E. faecium (n = 42, 5%), Escherichia coli (n = 21, 2.5%), and P. aeruginosa (n = 14, 1.7%). For CAUTI, Acinetobacter spp. was the most frequently isolated organism (n = 16, 22.2%), followed by Enterococcus faecalis (n = 13, 18%), E. faecium (n = 11, 15.3%), E. coli (n = 11, 15.3%), P. aeruginosa (n = 10, 15.3%), and K. pneumoniae (n = 7, 9.7%). Figures 1 and 2 illustrate the shifting trends in the prevalence of these organisms within the Neonatal intensive care unit (NICU) and critical care unit (CCU), the two ICUs of our institution, where the majority of HAIs were observed. Few cases of HAIs were also observed in Pediatric ICU (2.2% of CLABSI) and neonatal ICU (16.2% of Non CLABSI).
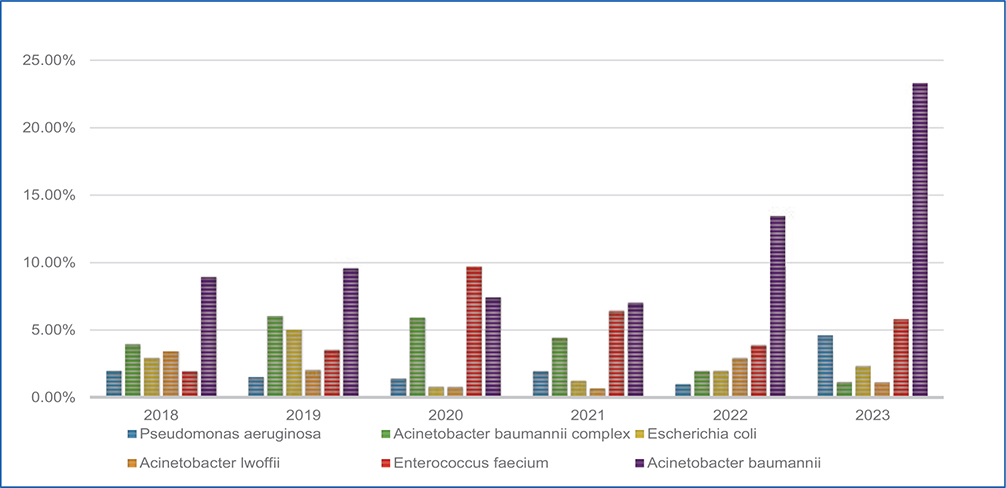
Figure 1. Trends in distribution of organisms in NICU (2018–2023).
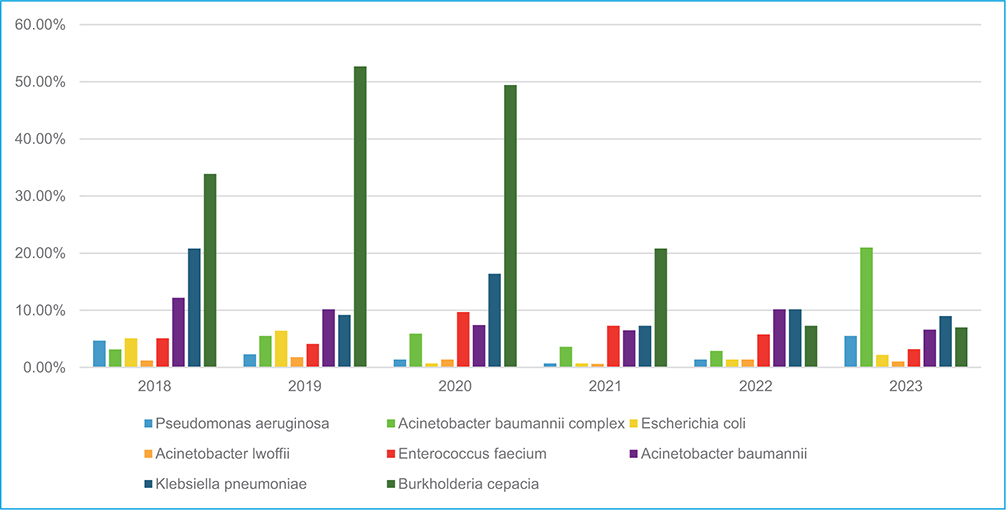
Figure 2. Trends in distribution of organisms in CCU (2018–2023).
Five-Year Antimicrobial Susceptibility Trends of Commonly Isolated HAI Pathogens (2018–2023): The data reveal a concerning degree of resistance across various antimicrobial classes, underscoring the escalating difficulty in managing infections caused by Gram-negative bacteria due to diminishing antibiotic efficacy. Figure 3 depicts the overall antimicrobial susceptibility trends of the major HAI pathogens from 2018 to 2023.
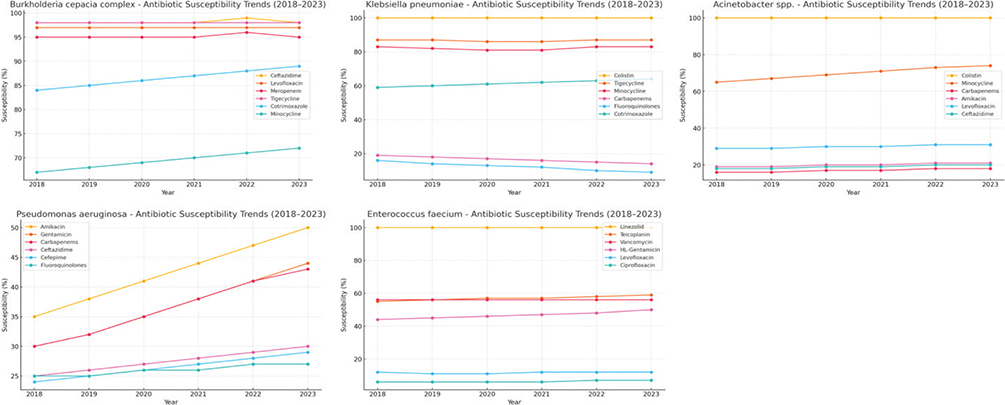
Figure 3. Antimicrobial susceptibility dynamics of major HAI pathogens over 5 years (2018–2023). HAI: healthcare-associated infections.
Burkholderia cepacia complex: Burkholderia cepacia demonstrated high sensitivity to levofloxacin (97%), ceftazidime (98%), meropenem (95%), cotrimoxazole (84%), tigecycline (98%), and minocycline (67%). Analysis of the susceptibility trends revealed a consistently high sensitivity of B. cepacia isolates to key antimicrobials throughout the study period. The organism showed high susceptibility to ceftazidime (mean 98%) and levofloxacin (mean 97%), with no statistically significant fluctuation (P > 0.1), reflecting sustained efficacy of these agents. Meropenem and tigecycline susceptibility also remained high (95 and 98%, respectively), while cotrimoxazole exhibited a mild upward trend (slope = +2.1, P = 0.087). Minocycline showed moderate variability (67–72%) without statistical significance. Overall, B. cepacia did not show evidence of progressive resistance over the 5-year period.
Klebsiella pneumoniae: Klebsiella pneumoniae isolates exhibited the highest susceptibility to colistin (100%), followed by Tigecycline (87.27%) and Minocycline (83.30%). However, low susceptibility was observed for fluoroquinolones such as levofloxacin (6.45%) and ciprofloxacin (16%), as well as cephalosporins such as ceftazidime (2.60%) and ceftriaxone (1.00%). Carbapenems, including imipenem (18.80%), meropenem (17.05%), and doripenem (20%), also showed poor susceptibility. Moderate susceptibility was observed for cotrimoxazole (58.73%) and gentamicin (47.41%). The susceptibility trends for K. pneumoniae isolates indicated a worrying decline across most antimicrobial classes. Carbapenem susceptibility (imipenem, meropenem, doripenem) showed a consistent downward trend (slopes ranging from –1.8 to –3.4; P < 0.05 for meropenem), underscoring an expanding burden of carbapenem resistance. Cephalosporins (ceftazidime, cefepime, ceftriaxone) exhibited the lowest effectiveness, remaining below 5% susceptibility across all years. In contrast, colistin showed 100% susceptibility throughout, with tigecycline and minocycline having high susceptibility levels of 87 and 83%, respectively. Moderate improvement was observed for cotrimoxazole (slope = +3.9, P = 0.072) and gentamicin (slope = +2.8, P = 0.089), but fluoroquinolones (levofloxacin, ciprofloxacin) remained largely ineffective (< 20% susceptibility).
Acinetobacter spp.: All Acinetobacter spp. isolates were found to be susceptible to colistin, with 71% also showing sensitivity to minocycline. However, susceptibility to other antibiotics, including levofloxacin (29%), ceftazidime (18%), imipenem (16%), cotrimoxazole (23%), amikacin (19%), cefepime (17%), ceftriaxone (8%), gentamicin (10%), meropenem (16%), and piperacillin/tazobactam (16%), was notably low. Colistin retained full activity (100%) across all study years. A statistically significant upward trend was observed for minocycline (slope = +2.31, P = 0.041), rising from 65 to 74% susceptibility. Other agents, including levofloxacin, amikacin, ceftazidime, and carbapenems (imipenem, meropenem), displayed modest increases (slopes +0.8 to +1.6) that were not statistically significant (P > 0.1). Cephalosporins (cefepime, ceftriaxone) and β-lactam/β-lactamase inhibitor combinations (piperacillin-tazobactam) showed low susceptibility of < 20% over 5 years.
Pseudomonas aeruginosa: Trend analysis of P. aeruginosa revealed moderate yet promising improvements in aminoglycoside and carbapenem susceptibility. Amikacin (slope = +3.21, P = 0.038) and gentamicin (slope = +2.94, P = 0.042) both showed significant upward trends, while meropenem (slope = +2.73, P = 0.054) and imipenem (slope = +3.10, P = 0.048) approached significance, suggesting gradually enhanced efficacy of these agents. Ceftazidime and cefepime exhibited modest gains (slopes +1.9 and +1.5, respectively) without statistical significance (P > 0.1). Fluoroquinolones (ciprofloxacin and levofloxacin) remained variably effective, with stable intermediate susceptibility (~25–30%) throughout.
Enterococcus faecium: For E. faecium, sensitivity rates were 100% for linezolid, 57% for teicoplanin, 56% for vancomycin, 44% for high-level gentamicin, 11.7% for levofloxacin, and 6% for ciprofloxacin. Linezolid and vancomycin, both show stable trends over time. Teicoplanin demonstrated a slight upward shift (slope = +1.6, P = 0.083), while high-level gentamicin resistance decreased modestly (slope = –2.1, P = 0.091), indicating gradual improvement in aminoglycoside synergy potential. Conversely, fluoroquinolone susceptibility (levofloxacin, ciprofloxacin) remained very low (< 15%) without significant year-to-year variation.
Discussion
HAIs, especially those resulting from the insertion of medical devices, pose a significant challenge for hospitals (11). Effective management of these infections is crucial for enhancing patient outcomes, particularly in ICUs where patients are at increased risk due to their severe underlying conditions and the frequent use of invasive devices. To address this issue, we conducted a comprehensive single-center study on CLABSI and CAUTI within the ICUs of a tertiary care facility in Northern India. Our study revealed an overall HAI rate of 12.85%, which is lower than some studies conducted in various states of India, such as those by Shalini et al. (27.4%) (12) and Singh et al. (17.6%) (13) but significantly higher than other Indian studies (4.62%) and international benchmarks (4.4%) (14). Additionally, our findings indicated that the incidence of HAIs were predominantly observed among adult patients, with a higher proportion in males. This observation aligns with the results of studies by Moolchandani et al. (15), Anand et al. (16), Patel et al. (17) and Mathur et al. (18). Notably, while the CLABSI rate at our hospital was higher, it remained comparable to other institutions (Table 5). However, the CAUTI rate was relatively lower. No CAUTI cases were recorded between 2020 and 2022. This coincided with the COVID-19 pandemic period, during which elective admissions were reduced. Intensive IPC reinforcement during pandemic control likely contributed to the observed zero rate.
| Source | CLABSI | CAUTI | |||||
| AIIMS, Delhi (19) | 7.2 | 15.1 | |||||
| Poland 2017 (20) | 8 | 3 | |||||
| INICC, 2003–2008, 25 developing countries (21) | 7.4 | 6.1 | |||||
| NHSN, 2006–2008, USA (22) | 2.1 | 3.4 | |||||
| KISS, 2004–2009, Germany (22) | 1.3 | 2.0 | |||||
| Army College of Medical Sciences and Base Hospital, Delhi Cantt (23) | 8.1 | 4.5 | |||||
| Present Study | 11 | 0.75 | |||||
| HAI: healthcare-associated infections; CLABSI: central line-associated bloodstream infections; CAUTI: Catheter-Associated Urinary Tract Infection. | |||||||
The median time to infection in CLABSI patients was approximately 10 days after ICU admission, while that for CAUTI was 9 days. These findings are consistent with the typical window of device-related infection acquisition described in previous literature, suggesting that prolonged indwelling device use and extended critical care stays remain major risk factors for HAIs (24). The median total LOS in the ICUs aligns with that in the literature (25). The 14-day and final outcomes revealed alarmingly high mortality rates among both CLABSI (40.9% at 14 days; 54.3% final) and CAUTI patients (58.3% at 14 days; 63.9% final), which aligns with the literature (26, 27).
The most frequently identified pathogen responsible for HAIs varies by region. In our study, B. cepacia was the predominant pathogen (n = 438, 52.3%), whereas in a study by Lohiya et al. in Central India, Acinetobacter spp. was the most commonly isolated pathogen (n=322, 77.4%) (14). This high prevalence of B. cepacia can be attributed to the outbreak of the organism during the study period (28). The incidence of HAIs differs markedly across various healthcare institutions and regions, underscoring the necessity of tailoring infection control strategies to specific contexts. This variability may be attributed to differences in infection control practices, patient demographics, healthcare infrastructure, and data collection methods. Our hospital experienced a high rate of HAIs, which can be linked to factors such as shortages of manpower, personal protective equipment (PPE), hand sanitizers, disposables, hand rubs, lack of motivation, insufficient training and educational sessions, inadequate standard operating procedures (SOPs) in the ICU, non-compliance with hand hygiene practices, and reluctance to modify habits. By addressing these issues through the FOCUS PDSA and root cause analysis strategies, we observed a significant reduction in HAI rates following the implementation of standardized IPC measures and improvements to existing protocols. In addition training sessions provided to the healthcare personnel under this global surveillance capacity building project, both at the individual level and via online platforms, proved to be of great help to curb the HAIs. The consequences of HAIs and antimicrobial resistance on patient outcomes are profound, with over 24% of patients affected by healthcare-associated sepsis and 52.3% of those treated in ICUs dying each year. The mortality rate doubles to triples when infections are resistant to antimicrobials. The study observed a mortality rate of 58.3%, which surpasses the crude mortality rates reported in the INICC survey for India, where figures ranged from 35.2 to 44.9% (21). Nonetheless, our device utilization ratios were aligned with those seen in studies from China, Malaysia, and Iran (22, 29, 30), with central lines and urinary catheters showing utilization ratios of 0.44 and 0.6, respectively.
The 5-year antimicrobial susceptibility trends highlight a concerning but heterogeneous resistance pattern among predominant HAI pathogens. Burkholderia cepacia maintained consistently high susceptibility across major agents, indicating minimal resistance evolution during the study period. In contrast, K. pneumoniae demonstrated extensive multidrug resistance, with persistently low susceptibility to carbapenems and cephalosporins, underscoring the dominance of carbapenem-resistant strains. Acinetobacter spp. exhibited sustained colistin susceptibility and a marginal improvement in minocycline sensitivity, yet remained highly resistant to most conventional antibiotics. Pseudomonas aeruginosa showed moderate but encouraging increases in aminoglycoside and carbapenem susceptibility, likely reflecting improved antimicrobial stewardship interventions. Among Gram-positive isolates, E. faecium retained full susceptibility to linezolid and partial sensitivity to vancomycin and teicoplanin, with persistently low fluoroquinolone efficacy. Collectively, these findings underscore the growing therapeutic challenge posed by MDR Gram-negative bacteria and reinforce the need for robust infection control and targeted antibiotic policy measures. These results are comparable with a recent study conducted in this region (31).
Conclusion and recommendations
This study underscores the critical importance of continuous surveillance, targeted interventions, and the exchange of knowledge to effectively reduce HAIs and enhance patient outcomes across diverse healthcare settings. Regular Utilization of the IPCAF Tool is essential to conduct regular assessments using the IPCAF (Infection Prevention and Control Assessment Framework) tool within the facility. Consistent application of this tool will help in evaluating the effectiveness of current infection control measures and identifying areas requiring improvement (32). This ongoing assessment ensures that infection control practices remain robust and adaptive to emerging challenges. Enhanced Training for IPC Personnel is a critical need to invest in the training of healthcare professionals. Enhancing the competency of these individuals through specialized training programs will equip them with the necessary skills to implement effective infection control strategies. Additionally, improving the nurse-to-patient ratio is essential to ensure that there is adequate oversight and care, reducing the likelihood of infection transmission. Implementation of HAI Prevention Bundles is crucial. These bundles should include strategies for preventing CLABSI, CAUTI, and promoting rigorous hand hygiene practices. By adhering to these evidence-based bundles, healthcare facilities can significantly reduce infection rates and improve patient outcomes. Quality improvement initiatives should be supported through targeted training and the provision of detailed guidance materials. Training programs should be designed to enhance the knowledge and skills of healthcare staff in implementing infection control measures. Providing up-to-date resources and guidance will facilitate continuous improvement and adherence to best practices. Effective and timely communication between the Microbiology and Clinical teams is vital for managing infections. Establishing regular channels of communication ensures that clinical decisions are taken based on microbiological data, leading to better patient management and more effective infection control. Adequate administrative support is necessary for the successful implementation of infection control measures. This includes allocating sufficient manpower and budgetary resources to support infection prevention initiatives. Administrative backing is essential for sustaining efforts and ensuring that infection control programs are well-resourced and effective. The availability and correct use of PPE such as gowns, masks, gloves, and caps must be prioritized. Ensuring that PPE is readily accessible and properly utilized by healthcare staff is fundamental to protecting both patients and healthcare workers from infections. Controlling Attendant Flow within the healthcare facility is important for reducing the risk of infection. Implementing strict visitor policies and managing the flow of individuals can help to minimize potential exposure and maintain a safer environment for patients. Adhering to Biomedical Waste Segregation Protocols is critical for infection control. Following established protocols for the disposal of infectious and hazardous materials ensures that waste is handled safely, thereby preventing cross-contamination and reducing the risk of infection spread. By implementing these recommendations, healthcare facilities can enhance their infection control practices and effectively reduce the incidence of HAIs, ultimately improving patient safety and outcomes. Monitoring HAIs in ICUs is crucial for enhancing treatment outcomes. This study highlights the pressing need for robust strategies to tackle the escalating menace of antimicrobial resistance within healthcare environments. It underscores the imperative for effective IPC protocols, the implementation of rigorous antibiotic stewardship programs, and the adoption of multifaceted surveillance approaches to counteract the burgeoning threat of MDR organisms.
Limitations
Firstly, this surveillance was restricted to bloodstream and urinary tract device-associated infections; hospital-acquired and VAP were not included. Secondly, although data collection was prospective and standardised, patient-level variables such as comorbidities, illness severity (acute physiology and chronic health evaluation [APACHE II] and sequential organ failure assessment [SOFA] scores), and prior antibiotic exposure were not consistently recorded, limiting multivariate risk-factor analysis and adjustment for potential confounders. Thirdly, the study was conducted at a single tertiary-care centre, which may limit generalizability to other settings with differing infrastructure and infection-control resources.
Acknowledgments
The authors would like to thank Dr. Purva Mathur and the AIIMS, New Delhi team, Dr. Kamini Walia and the ICMR team, Paul Malpiedi, Daniel VanderEnde, Siromany Valan (U.S. Centers for Disease Control and Prevention) for their assistance with this capacity building project.
Authors’ contributions
B.A.F. conceived the study design and methodology, supervised the research and contributed to writing and editing the manuscript draft. S.N. and S.B. conducted the data collection and analysis and curated the data. U.Q. and S.J.W. curated the data, wrote the manuscript’s first draft, and did the literature review and editing. A.S. and A.W.M. contributed to the clinical aspect of the research. M.A. and G.B. assisted in writing and editing the manuscript. All the authors have approved the final draft.
Ethics approval
All procedures adhered to the ethical standards of the Indian Council of Medical Research (ICMR) guidelines on human experimentation and conformed to the principles outlined in the Declaration of Helsinki (1975, revised 2013). This study was approved by the ethical committee of Sher-i-Kashmir Institute of Medical Sciences (SKIMS) under SIMS 131/IEC-SKIMS/2022-95.
References
| 1. | World Health Organization. Global report on infection prevention and control. Available from: https://www.who.int/publications/i/item/9789240051164 [cited 22 March 2025]. |
| 2. | Erdem I, Yıldırım I, Arar C. A 5-year surveillance of healthcare-associated infections in a university hospital: a retrospective analysis. SAGE Open Med 2022; 10: 1–8. doi: 10.1177/20503121221091789 |
| 3. | Li RJ, Wu YL, Huang K, Hu XQ, Zhang JJ, Yang LQ, et al. A prospective surveillance study of healthcare-associated infections in an intensive care unit from a tertiary care teaching hospital from 2012–2019. Medicine (Baltimore) 2023; 102(31): e34469. doi: 10.1097/MD.0000000000034469 |
| 4. | Szabó S, Feier B, Capatina D, Tertis M, Cristea C, Popa A. An overview of healthcare-associated infections and their detection methods caused by pathogen bacteria in Romania and Europe. J Clin Med 2022; 11(11): 3204. doi: 10.3390/jcm11113204 |
| 5. | Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of healthcare-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control 2008; 36(5): 309–32. doi: 10.1016/j.ajic.2008.03.002 |
| 6. | Johnson NB, Hayes LD, Brown K, Elizabeth CH, Ethier KA. CDC National Health Report: leading causes of morbidity and mortality and associated behavioural risk and protective factors–United States, 2005–2013. MMWR Suppl 2014; 63(4): 3–27. |
| 7. | Magill SS, O’Leary E, Janelle SJ, Thompson DL, Dumyati G, Nadle J, et al. Changes in prevalence of health care–associated infections in U.S. hospitals. N Engl J Med 2018; 379(18): 1732–44. doi: 10.1056/NEJMoa1801550 |
| 8. | Sikora A, Zahra F. Nosocomial infections. Treasure Island, FL: StatPearls Publishing; 2025 [updated 2023 Apr 27]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK559312/ [cited 22 March 2025] |
| 9. | Van Duin D, Paterson DL. Multidrug-resistant bacteria in the community: trends and lessons learned. Infect Dis Clin North Am 2016; 30: 377–90. doi: 10.1016/j.idc.2016.02.004 |
| 10. | Arzilli G, De Vita E, Pasquale M, Carloni LM, Pellegrini M, Di Giacomo M, et al. Innovative infection control and surveillance techniques in hospital settings and long-term care facilities: a scoping review. Antibiotics 2024; 13: 77. doi: 10.3390/antibiotics13010077 |
| 11. | Singh S, Pandya Y, Patel R, Paliwal M, Wilson A, Trivedi S. Surveillance of device-associated infections at a teaching hospital in rural Gujarat – India. Indian J Med Microbiol 2010; 28(4): 342–7. doi: 10.4103/0255-0857.71830 |
| 12. | Shalini S, Kranthi K, Gopalkrishna Bhat K. The microbiological profile of nosocomial infections in the intensive care unit. J Clin Diagn Res 2010; 4: 3109–12. |
| 13. | Singh S, Chaturvedi R, Garg SM, Datta R, Kumar A. Incidence of healthcare associated infection in the surgical ICU of a tertiary care hospital. Med J Armed Forces India 2013; 69(2): 124–9. doi: 10.1016/j.mjafi.2012.08.028 |
| 14. | Lohiya R, Deotale V. Surveillance of health-care associated infections in an intensive care unit at a tertiary care hospital in Central India. GMS Hyg Infect Control 2023; 18: Doc28. |
| 15. | Moolchandani K, Sastry AS, Deepashree R, Sistla S, Harish BN, Mandal J. Antimicrobial resistance surveillance among intensive care units of a tertiary care hospital in Southern India. J Clin Diagn Res 2017; 11(2): DC01–7. doi: 10.7860/JCDR/2017/23717.9247 |
| 16. | Anand N, Nayak IM, Advaitha MV, Thaikattil NJ, Kantanavar KA, Anand S. Antimicrobial agents’ utilization and cost pattern in an intensive care unit of a teaching hospital in South India. Indian J Crit Care Med 2016; 20(5): 274–9. doi: 10.4103/0972-5229.182200 |
| 17. | Patel MK, Barvaliya MJ, Patel TK, Tripathi C. Drug utilization pattern in critical care unit in a tertiary care teaching hospital in India. Int J Crit Illn Inj Sci 2013; 3(4): 250–5. doi: 10.4103/2229-5151.124128 |
| 18. | Mathur P, Malpiedi P, Walia K, Srikantiah P, Gupta S, Lohiya A, et al. Health-care-associated bloodstream and urinary tract infections in a network of hospitals in India: a multicentre, hospital-based, prospective surveillance study. Lancet Glob Health 2022; 10(9): e1317–25. doi: 10.1016/S2214-109X(22)00274-1 |
| 19. | Mathur P, Tak V, Gunjiyal J, Nair SA, Lalwani S, Kumar S, et al. Device-associated infections at a level-1 trauma centre of a developing nation: impact of automated surveillance, training and feedbacks. Indian J Med Microbiol 2015; 33(1): 51–62. doi: 10.4103/0255-0857.148378 |
| 20. | Kołpa M, Wałaszek M, Gniadek A, Wolak Z, Dobroś W. Incidence, microbiological profile and risk factors of healthcare-associated infections in intensive care units: a 10 year observation in a provincial hospital in Southern Poland. Int J Environ Res Public Health 2018; 15(1): 112. |
| 21. | Ramasubramanian V, Iyer V, Sewlikar S, Desai A. Epidemiology of healthcare acquired infection – an Indian perspective on surgical site infection and catheter related blood stream infection. Ind J Basic Appl Med Res 2014; 3(4): 46–63. |
| 22. | Rai V, Rosenthal V, Gan CS, Rosenthal VD, González Flores HA, Pazmiño L, et al. Device-associated infection and mortality rates, bacterial resistance, and length of stay in hospitals of Malaysia: international nosocomial infection. Can J Infect Contr 2016; 31(2): 107–12. |
| 23. | Khan ID, Basu A, Kiran S, Trivedi S, Pandit P, Chattoraj A. Device-associated healthcare-associated infections (DA-HAI) and the caveat of multiresistance in a multidisciplinary intensive care unit. Med J Armed Forces India 2017; 73(3): 222–31. doi: 10.1016/j.mjafi.2016.10.008 |
| 24. | Sleziak J, Błażejewska M, Duszyńska W. Catheter-associated urinary tract infections in the intensive care unit during and after the COVID- 19 pandemic. BMC Infect Dis 2025; 25(1): 595. doi: 10.1186/s12879-025-10996-2 |
| 25. | Hasan B, Bechenati D, Bethel HM, Cho S, Rajjoub NS, Murad ST, et al. A systematic review of length of stay linked to hospital-acquired falls, pressure ulcers, central line-associated bloodstream infections, and surgical site infections. Mayo Clin Proc Innov Qual Outcomes 2025; 9(3): 100607. doi: 10.1016/j.mayocpiqo.2025.100607 |
| 26. | Mosquera JMA, Assis Reveiz JK, Barrera L, Liscano Y. Impact of central line-associated bloodstream infections on mortality and hospital stay in adult patients at a Tertiary Care Institution in Cali, Colombia, 2015–2018. J Clin Med 2024; 13(18): 5376. doi: 10.3390/jcm13185376 |
| 27. | Parveen R, Thakur AK, Srivastav S, Puraswani M, Srivastava AK, Chakrabarti A, et al. Profile of central line-associated bloodstream infections in adult, paediatric, and neonatal intensive care units of hospitals participating in a health-care-associated infection surveillance network in India: a 7-year multicentric study. Lancet Glob Health 2025; 13(9): e1564–73. doi: 10.1016/S2214-109X(25)00221-9 |
| 28. | Fomda B, Velayudhan A, Siromany VA, Bashir G, Nazir S, Ali A, et al. An outbreak of Burkholderia cepacia bloodstream infections in a tertiary-care facility in northern India detected by a healthcare-associated infection surveillance network. Infect Control Hosp Epidemiol 2023; 44(3): 467–73. doi: 10.1017/ice.2022.111 |
| 29. | Wang L, Zhou KH, Chen W, Yu Y, Feng SF. Epidemiology and risk factors for nosocomial infection in the respiratory intensive care unit of a teaching hospital in China: a prospective surveillance during 2013 and 2015. BMC Infect Dis 2019; 19(1): 145. doi: 10.1186/s12879-019-3772-2 |
| 30. | Masoudifar M, Gouya MM, Pezeshki Z, Eshrati B, Afhami S, Farzami MR, et al. Health care-associated infections, including device-associated infections, and antimicrobial resistance in Iran: the national update for 2018. J Prev Med Hyg 2022; 62(4): E943–9. |
| 31. | Fomda BA, Qadri U, Bashir G, Qadri SM, Nazir SS, Hakak I. Superbug surge: a tale of seven-year battle against escalating antimicrobial resistance in North India. Curr Microbiol 2025; 82: 340. doi: 10.1007/s00284-025-04321-y |
| 32. | Katyal S, Srivastav S, Katoch O, Rodrigues C, Rupali P, Chakrabarti A, et al. A self-reported survey on the implementation of infection prevention and control elements in Indian hospitals, part of a HAI surveillance network: results from 23 hospitals conducting a standardized IPC assessment. Am J Infect Control 2023; 51(1): 29–34. doi: 10.1016/j.ajic.2022.04.014 |