ORIGINAL ARTICLE
Alcoholic preparation for hand hygiene in ophthalmic day hospitals: an applied research
Thalita Souza Santos* and Roberta Costa
Federal University of Santa Catarina, Florianopolis, SC, Brazil
Abstract
Objective: To define and validate the optimal consumption of alcoholic preparation for ophthalmic day hospitals based on the minimum opportunities for hand hygiene (HH) required during the care provided in the Diagnostic Imaging Center and the Surgical Center of an ophthalmic day hospital.
Method: An applied research was developed between May and July 2021. To conduct the research, six phases were defined: 1) Establishment of the conceptual structure; 2) Mapping the minimum opportunities for HH; 3). Validation of the mapping of minimum opportunities; 4). Calculation of the ideal minimum consumption of alcoholic preparation for HH; 5) Comparison of results with the institution’s data. 6). Development of the guide. Nineteen health professionals participated in this study between the validation stages in the institution and validation with specialists.
Results: We identified that the minimum consumption of alcoholic preparation is: 63 mL/surgical patient undergoing local anesthesia, 126 mL/surgical patient submitted to local anesthesia with sedation, 123 mL/surgical patient submitted to general anesthesia, 15 mL/patient submitted to unprepared examination, 21 mL/patient submitted to prepared examination, and 57 mL/patient submitted to examination with contrast.
Discussion: The profile of the patient, the institution, and the care provided may directly influence the number of opportunities for HH, which, in turn, directly impacts the reference of alcohol preparation consumption. Therefore, a single goal cannot translate the need for all of them. This condition refers to the need to determine specific consumption goals by patient profile and procedure so that the alcohol preparation consumption indicator effectively reflects the quality of care achieved in HH.
Keywords: nursing; hand hygiene; local anti-infectives; eye health services; infection control
Citation: Int J Infect Control 2026, 22: 23810 – http://dx.doi.org/10.3396/ijic.v22.23810
Copyright: © 2026 Thalita Souza Santos and Roberta Costa. This is an Open Access article distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material for any purpose, even commercially, provided the original work is properly cited and states its license.
Received: 16 October 2024; Revised: 11 September 2025; Accepted: 21 September 2025; Published: 4 March 2026
Competing interests and funding: The author reports no conflict of interests and funding.
*Thalita Souza Santos, Universidade Federal de Santa Catarina, Florianópolis, SC, Brasil, Email: thallith@yahoo.com.br
Currently, hand hygiene (HH) is among the most widespread strategies for preventing infections. Although HH practices are simple and directly associated with reduced infection rates in healthcare services, adherence among professionals remains low, posing a challenge for infection control (1). In Brazil, recorded HH adherence rates averaged between 8.5 and 54.2% (2).
The World Health Organization (WHO) internationally released the Multimodal Strategy to improve adherence to HH practices (3), which brought one of the pillars as ‘5 Moments for Hand Hygiene’ consisting of directing the main moments when HH is necessary, namely: 1) Before touching the patient; 2) Before performing a clean/aseptic procedure; 3) After the risk of exposure to bodily fluids or excretions; 4) After touching the patient; 5) After touching surfaces close to the patient (4, 5).
Another recommendation is to provide easy access to alcoholic preparation for HH at the point of patient care (3). At the time, the use of alcoholic preparations was ratified as a standard procedure for HH in place of washing hands with soap and water when they are not visibly dirty or contaminated with organic matter (6). Therefore, the availability of alcoholic preparation in an easily accessible place for professionals became mandatory in Brazil as per the publication of the Collegiate Board Resolution (RDC) No. 42 in 25 October 2010 (7).
The WHO also recommends predicting indicators that enable the measurement of adherence to HH practices directly and indirectly. The mandatory indicators are the consumption of alcoholic preparation for hands and the consumption of soap. The recommended indicator is the percentage (%) of adherence to HH (number of HH actions performed by health professionals/number of opportunities that occurred for HH, multiplied by 100) (4, 5). Each health institution, according to its routine, can define the method for collecting information on consumption. It is recommended that the products be made available at the point of patient care for immediate use (8), and the recommended quantity is 20 mL per patient per day, according to the 2010 Hand Hygiene Self-Assessment Framework published by WHO (3).
Given that there is currently no guidance on the profile for applying the reference published by the WHO in the different health institutions, the validation of the alcoholic solution consumption indicator for HH was not performed (9).
This study aimed to define how to calculate the optimal alcoholic preparation consumption for HH for ophthalmic day hospitals based on the minimum opportunities available during the care provided in the Diagnostic Imaging Center (DIC) and Surgical Center (SC) and to prepare a guideline for institutions on how to define and monitor alcoholic preparation consumption for HH.
Methods
We applied a research with a quantitative and qualitative approach developed in the context of an ophthalmological hospital in southern Brazil. To ensure methodological rigor, different data collection and analysis strategies were developed to evaluate the investigation context and obtain the best results properly. This study was approved by the Research Ethics Committee under the protocol number CAAE 42606321.0.0000.0121, with the consolidated opinion No. 4,590,692 issued on March 15, 2021.
This study was conducted in six phases: 1) Establishment of the conceptual structure (Integrative Literature Review); 2). Mapping the minimum opportunities for HH related to the profile of patients treated in an ophthalmic day hospital; 3). Validation of the mapping of minimum opportunities (Content Validation); 4). Calculation of the ideal minimum consumption of alcoholic preparation for HH; 5). Comparison of results with the institution’s data. 6). Development of protocol to guide other institutions to define the minimum consumption of alcoholic preparation based on their reality.
Thus, an integrative literature review was conducted. The research question is what is the information available in the literature to define the value of alcoholic preparation consumption for HH in health institutions? Studies published as events/congresses, technical materials, and articles from the following Coordination for the Improvement of Higher Education Personnel (CAPES) journal databases (www.periodicos.capes.gov.br) were selected: Scopus; Web of Science; Scientific Electronic Library Online (SciELO); PubMed/Medline; CINAHL – Cumulative Index to Nursing and Allied Health Literature; BDENF – Nursing Database; and LILACS – Latin American and Caribbean Health Sciences Literature, through the Virtual Health Library: BVS (BIREME).
To perform search in the databases, the following keywords were chosen according to the structured and multilingual vocabulary DeCS – Health Sciences Descriptors: ‘Patient Safety’, ‘Hand Hygiene’, ‘Local Anti-Infectives’. The inclusion criteria were articles in Portuguese, English, and Spanish with content available in full, online, and free of charge, published between 2010 and 2021, and agreed with the pre-established theme.
For the selection, the analysis was performed following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) methodology. We conducted the analysis by thoroughly reading titles and abstracts to select studies that met the defined inclusion criteria and were relevant to the proposed objective. PleasFinally, five articles were selected that addressed the theme, one of which dealt with the number of milliliters to be used for an adequate HH, two on the consumption of alcohol preparation for HH identified in the institutions, and two had information related to both analytical categories.
Subsequently, mapping the minimum HH opportunities in the care processes of patients treated in the SC and DIC was conducted through a collection of documentary data in the institution’s directory regarding the workflows, Standard Operating Procedures (SOPs), and clinical protocols of these departments. The opportunities were mapped according protocol recommended by the WHO in relation to the ‘5 Moments for Hand Hygiene’ following the logic of processes described (Fig. 1).
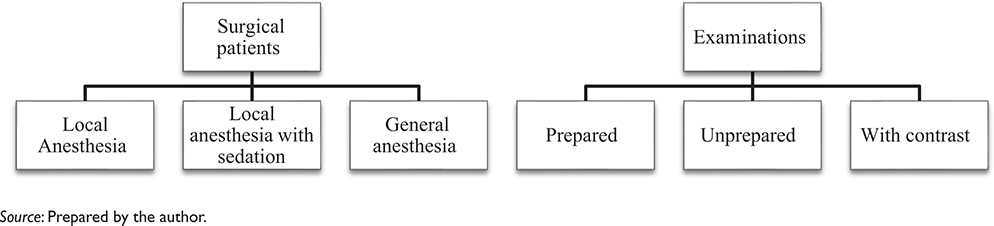
Fig. 1. Profiles for mapping the minimum HH opportunities by processes.
Next, a meeting was organized to review and indicate the necessary adjustments to the mapping, which was reliable. The researcher used a script with the objective, steps to be performed in the meeting, and the expected result, which served as support for planning and developing activities. The researchers also prepared a Microsoft PowerPoint presentation addressing the research objective, its importance, and methodology. The meeting took place in June 2021. All nursing leaders from the institution were invited (N=5), including 2 nurses from the CC, 1 administrative nurse, 1 nurse, and 1 nursing technician (similar to an Licensed Practical Nurse in the United States of America) from the Diagnostic Imaging Center. Four professionals participated in this stage, having provided informed consent after reading the Informed Consent Form (ICF).
In the third stage, we validated the mapping of minimum opportunities for HH for each previously defined patient profile, as shown in Fig. 1. Two self-instructed questionnaires were prepared, one on the SC and the other on the DIC, containing an explanatory video with the guidelines for completing and properly judging the proposed questions. The mappings were presented in the form of flows to facilitate understanding. Participants were also informed through the explanatory video that the sequence in which the opportunities appeared was irrelevant, and only the total minimum number of opportunities mattered.
The questions had a score on a Likert scale for the judges to inform the agreement and fields to suggest the inclusion or withdrawal of any HH opportunity. To verify the validity of the content of the minimum opportunities described in this study, we used a minimum agreement of 0.80.
To create the validation committee, it was defined that nurses with experience in ophthalmic SC or DIC would be invited to work in the group of ophthalmic hospitals where the researchers are working, requiring a minimum of five participants to evaluate each sector. This stage was developed in June and July 2021.
A total of 32 nurses were invited to the committee of judges to validate the mappings. The professionals were invited to create the committee of judges through an existing group in a communication application of which the researcher is also part, where the objective, the research question, the importance of the theme, and the form of participation were explained. An FICF was obtained from all the participants, and a link to the evaluation questionnaires was made available to the participants through the Google Forms tool.
Regarding the form on the mapping of the SC, 8 nurses responded. These professionals are from several states of the country, with representatives from the South, Southeast, Midwest, and Northeast regions. This point is important as it increases the representativeness and, consequently, the reliability of the mapping, considering different realities. We also identified that most of them (N = 6) presented with 2 years or more of experience in ophthalmological SC.
Regarding the DIC mapping form, 12 managers of Diagnostic Imaging Centers were invited, of which 7 responded to the form on the mapping of minimum HH opportunities. These professionals also represented several cities and states of the country. Regarding the time of experience in ophthalmic DIC, all the participants (100%) presented with 2 years or more experience. The participation of DIC nurses by state was as follows: two from Rio de Janeiro, two from São Paulo, and three from Bahia.
Data were analyzed using the Content Validity Index (CVI). This index measures the rate (or percentage) of evaluators who agree with certain aspects of mapping. The index score is calculated by adding the number of items evaluated in ‘3’ or ‘4’. Items receiving a score of ‘1’ or ‘2’ have been reviewed or deleted. The formula used was the sum of answers ‘3’ or ‘4’ divided by the total number of answers (10).
Following this step, the reference results obtained in the research on minimum ideal consumption of alcoholic preparation for HH were crossed with the consumption data of one of the participants’ institutions. The institutional indicators managed by the Infection Prevention and Control Committee (IPC Committee) related to the consumption of alcohol and soap for HH for 2021 were analyzed. It was found that consumption monitoring is conducted by changing the alcohol refills in the dispensers of the critical sectors, currently being monitored by the Surgical Block, the Diagnostic Imaging Centers, and the Medical Offices. Data collection is conducted in partnership with the Sanitation team, which, by filling out standardized forms, informs the exchange of alcohol and soap refills monthly. The data on patient volume in the sectors are obtained by computerized reports via the institution’s operating system and entered in an Excel spreadsheet with calculation formulas, where it is possible to obtain the monthly consumption per patient-day.
Results
The results of the literature review conducted by the author made it possible to identify that the number of milliliters (mL) of alcoholic preparation for each HH has the average volume predicted for a correct procedure of 3 mL. However, it should be noted that for individuals with large hands, this volume may be inadequate (11). When evaluating the findings on the average consumption of alcoholic preparation per patient/day, we can see the prevalence of studies in general hospitals, with the classification of sectors in Intensive Care Unit (ICU) and non-Intensive Care Unit (non-ICU), which may be related to the fact that high complexity patients require more care and interventions than the others. Notably, none of the authors cited the target of 20 mL/patient/day recommended by the WHO in the document Hand Hygiene Self-Assessment Framework 2010 (4).
In the review meeting of the mapping with the nursing team of the institution, the minimum opportunities for HH in the SC and DIC for each type of patient served were discussed. The opportunities defined after the discussion are presented in figures 2 to 7.
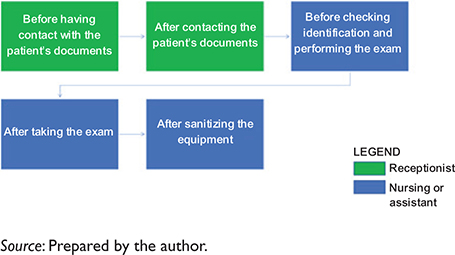
Fig. 2. Mapping of minimum HH opportunities per patient of the DIC with unprepared pupil examination.
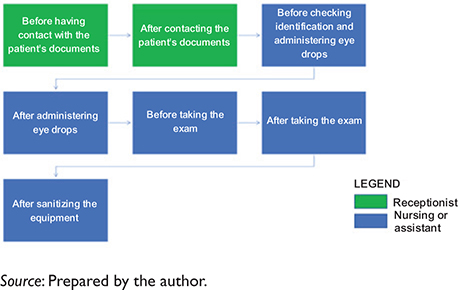
Fig. 3. Mapping of minimum HH opportunities per patient of the DIC with prepared pupil examination.
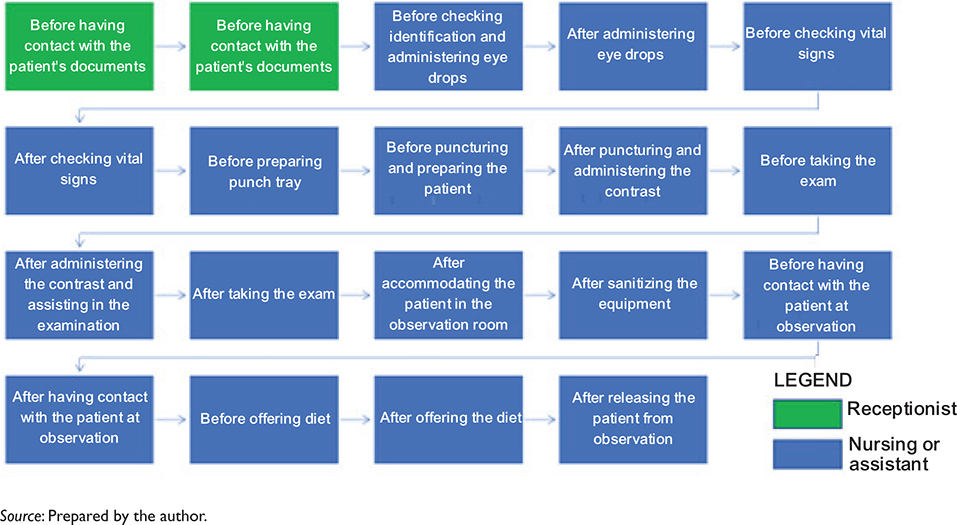
Fig. 4. Mapping of minimum HH opportunities per patient of the DIC in which contrast is administered (angiofluoresceinography).

Fig. 5. Mapping of minimum HH opportunities per patient of the SC undergoing local anesthesia.
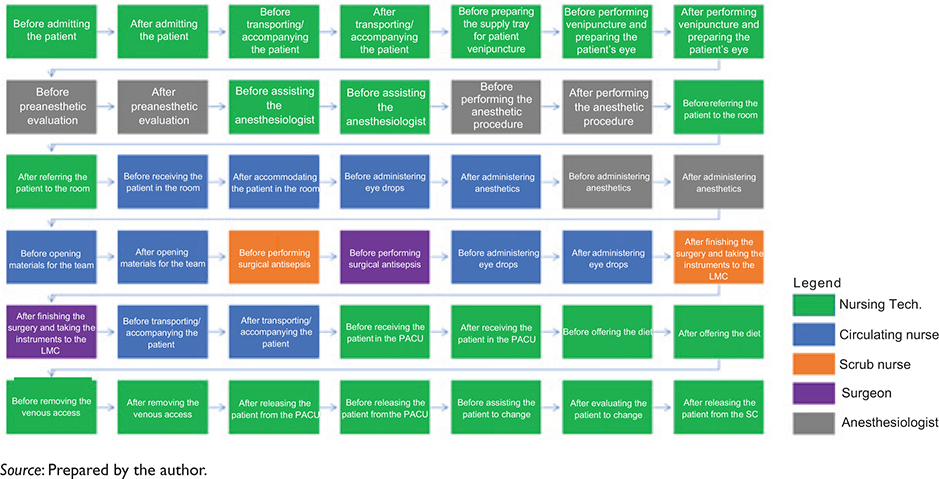
Fig. 6. Mapping of minimum HH opportunities per patient of the SC undergoing local anesthesia with associated sedation.

Fig. 7. Mapping of minimum HH opportunities per patient of the SC undergoing general anesthesia.
We continue validating the SC mapping by the 8 expert judges. By analyzing the levels of agreement in relation to the questions asked, it is revealed that all items had a CVI of greater than or equal to 0.80. It is noteworthy that no level of disagreement was indicated among the participants in all points presented. For the DIC mappings, all items had a CVI of greater than or equal to 0.80, and no level of disagreement was signaled between the participants. The evaluation results can be seen in Table 1.
| Question | CVI CC* | CVI DIC+ |
| This mapping adequately expresses the care process used in your institution, regardless of the sequence of events. | 1.0 | 1,0 |
| The hand hygiene (HH) opportunities highlighted in the mapping adequately express the minimum opportunities found in the process used in your institution, regardless of the sequence presented. | 1.0 | 1,0 |
| The total minimum HH opportunities for this patient profile are 7 times, with 5 per examination to be performed. | 1.0 | 1,0 |
| This mapping adequately expresses the care process used in your institution, regardless of the sequence of events. | 1.0 | 1,0 |
| The HH opportunities highlighted in the mapping adequately express the minimum opportunities found in the process used in your institution, regardless of the sequence presented. | 1.0 | 1,0 |
| The total minimum HH opportunities for this patient profile is 5 times, with 3 for each examination to be performed. | 1.0 | 1,0 |
| This mapping adequately expresses the care process used in your institution, regardless of the sequence of events. | 0.8 | 0,9 |
| The HH opportunities highlighted in the mapping adequately express the minimum opportunities found in the process used in your institution, regardless of the sequence presented. | 0.8 | 0,9 |
| The total number of minimum HH opportunities for this patient profile is 19 times, of which, 17 are related to the examination. | 1.0 | 1,0 |
| Legend: *Surgical Center; +Diagnostic Imaging Center. | ||
Regarding the DIC mappings, analysis of the agreement levels revealed that all items had a Content Validity Index (CVI) of 0.80 or higher. It was observed that there was also no level of disagreement among the participants in all points presented.
After the validation stage of mapping, the minimum opportunities for HH and the alcohol preparation consumption per patient profile served in the evaluated sectors were calculated in relation to these opportunities. According to the validated mappings, we found the total minimum HH opportunities by patient profile, which is shown in Table 2.
To determine the average volume of alcoholic preparation required for HH, we used data from the integrative literature review – where the average volume predicted for an appropriate procedure is around 3 mL (11–13). Voniatis (14) stated that ‘the coverage achieved is strongly correlated with hand size. However, an applied volume of 3 mL proved to be sufficient for most HH events (84%)’. Based on these assumptions, the calculation was followed by the formula: Average alcoholic preparation for HH (mL) multiplied by the total minimum opportunities for HH. The results obtained are presented in Table 3.
In July 2021, the reference results obtained in the research on minimum ideal alcoholic preparation for HH were crossed with the institution’s consumption data provided by the Infection Prevention and Control Committee (IPC Committee). The averages of alcohol and soap consumption per patient-day obtained between January and May 2021 are presented in Table 4.
After the analysis, we proceeded with structuring a guide to enable the findings to be replicated in other ophthalmological services. The document has the references for determining the minimum consumption of alcoholic preparation for HH according to this study, the description of the procedures of data collection, completion of the forms, and how to calculate the consumption of alcoholic preparation for HH in the ophthalmic SC and DIC.
Discussion
The results of this study allowed identifying an indicator of minimum consumption of alcoholic preparation for HH for ophthalmic day hospitals based on the minimum opportunities required during the care provided in the Diagnostic Imaging Center and the Surgical Center. When comparing the average data of current alcohol consumption with the volume of consumption predicted by assessing the minimum opportunities of HH, a considerable difference is perceived, even when associating the volume of soap, which can also be used for HH. The difference is 54.79 mL for the surgical patient and 14.21 mL for the examination patient, both in relation to the mapped profile with fewer opportunities for HH (SC: Local Anesthesia; DIC: Unprepared).
These findings are consistent with those reported by Brouqui and Aladro (15) in a letter to the editor published in 2016, where, through a radio frequency system for continuous monitoring of HH, they identified that for the monitored sector, with 15 rooms, the consumption of alcoholic preparation for HH was 7.48 times higher than the volume recommended by the French national objectives (20 mL/patient/day, as the WHO standard). They further state that ‘alcohol consumption for HH in the medical ward should be at least three times higher than currently recommended’, and that ‘the consumption objectives of the requested solution need to be quickly revisited for a more ambitious goal’ (15).
No other articles were found addressing the validation of the goal proposed by the WHO and by French standards, which highlights the need for further studies with a focus on sector and/or patient profiles, bringing more assertive objectives to infection control committees and their institutions.
It is concluded that the ideal minimum consumption of alcoholic preparation for ophthalmic day hospitals is linked to the number of minimum opportunities for HH, based on the 5 Moments for HH proposed by the WHO, ranging from 63 to 123 mL/patient in the SC and between 15 and 57 mL/patient in the DIC, according to the profile.
Health institutions face challenges in increasing the adherence of professionals to HH, and direct and indirect monitoring indicators are important to measure the effectiveness of the actions taken and their impact on the prevention of healthcare-related infections. For this, references on the adequate consumption of alcoholic preparation should be studied and substantiated according to the sector and/or profile of the patient attended, providing adequate parameters to achieve optimal adherence.
We found a minimum consumption reference proposed by the WHO, 20 mL/patient/day, in the literature. However, the studies show different consumption depending on the type of service/sector, and no records were found justifying standardization as a worldwide reference. There were also no records demonstrating the calculation used to get to this value, which decreases the reliability of this reference. The limitation of this study was the review by language, period, and articles with open access only.
Conclusion
Therefore, there is a need to review this concept with more robust studies that consider the specificities of each sector considering the number of minimum HH opportunities, making it possible to determine specific consumption goals by patient profile and procedure so that the alcohol preparation consumption indicator effectively reflects the quality of care achieved in HH. This issue requires broader discussion at both the national and international levels.
References
| 1. | Heisner K, Layell J, Citronberg R, Sampson M, Passaretti C, Skelton L. Beyond the hospital doors: challenges and insights from a multi-state healthcare system outpatient infection prevention program. Infect Contr Hosp Epidemiol. 2025; 46(4): 439–41. doi: 10.1017/ice.2024.232 |
| 2. | Mota APA, Costa EAM. Adhering to hand hygiene in Brazilian hospital services: a review study. Rev Saúde e Desenvolv 2023; 12(4): e41066. doi: 10.33448/rsd-v12i4.41066 |
| 3. | World Health Organization. Hand hygiene self-assessment framework 2010. Geneva: WHO; 2010. Available from: https://www.who.int/gpsc/country_work/hhsa_framework_October_2010.pdf [cited 23 December 2020]. |
| 4. | World Health Organization. Guide to implementation: a guide to implementing the WHO multimodal strategy for improving hand hygiene. Geneva: WHO; 2008. Available from: https://www.who.int/publications/i/item/a-guide-to-the-implementation-of-the-who-multimodal-hand-hygiene-improvement-strategy [cited 23 December 2020]. |
| 5. | Brasil. Portaria nº 1.377, de 9 de julho de 2013. Aprova os Protocolos de Segurança do Paciente. Brasília (DF): Ministério da Saúde; 2013. Available from: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2013/prt1377_09_07_2013.html [cited 28 August 2019]. |
| 6. | Fofanah BD, Kamara IF, Kallon C, Kamara RZ, Nuwagira I, Musoke R, et al. Evaluating the tolerability and acceptability of a locally produced alcohol-based handrub and hand hygiene behaviour among health workers in Sierra Leone: a longitudinal hospital-based intervention study. BMC Health Serv Res. 2024; 24: 940. doi: 10.1186/s12913-024-11368-3 |
| 7. | Brasil. Agência Nacional de Vigilância Sanitária. Resolução nº 42, de 25 de outubro de 2010. Dispõe sobre a obrigatoriedade de disponibilização de preparação alcoólica para fricção antisséptica das mãos pelos serviços de saúde do País, e dá outras providências. Brasília (DF): ANVISA; 2010. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/anvisa/2010/res0042_25_10_2010.html [cited 23 December 2020]. |
| 8. | Abdelmonem M, Abdelfattah MS, Alzehmi A, Alzaabi R, Alhosani H, Tanous J, Abdulrazzaq NM. Evaluation of electronic hand hygiene monitoring systems in UAE hospitals. Am J Clin Pathol 2024; 162: S117. doi: 10.1093/ajcp/aqae129.259 |
| 9. | Santos TS, Costa R. Consumo de preparação alcoólica para higienização das mãos em ambulatórios e Hospitais-Dia: revisão integrativa. Revista de Epidemiologia e Controle de Infecção 2023; 13(2): 44–53. doi: 10.17058/reci.v13i2.18042 |
| 10. | Correro-Bermejo A, Bas-Sarmiento P, Romero-Sánchez JM, Paloma-Castro O, Poza-Méndez M, Fernández-Gutiérrez M. Role of the health literacy assessment in healthcare: content validation of “Health Literacy Behaviour” nursing outcome. Int J Nurs Knowl 2024; 36(3): 264–74. doi: 10.1111/2047-3095.12482 |
| 11. | Bánsághi S, Soule H, Guitart C, Pittet D, Haidegger T. Critical reliability issues of common type alcohol-based handrub dispensers. Antimicrob Resist Infect Contr 2020; 9(1): 90. doi: 10.1186/s13756-020-00735-4 |
| 12. | Szabó R, Morvai J, Bellissimo-Rodrigues F, Pittet D. Use of hand hygiene agents as a surrogate marker of compliance in Hungarian long-term care facilities: first nationwide survey. Antimicrob Resist Infect Control. 2015; 4: 32. doi: 10.1186/s13756-015-0069-0 |
| 13. | Hansen S, Schwab F, Gastmeier P, PROHIBIT Study Group, Pittet D, Zingg W, et al. Provision and consumption of alcohol-based hand rubs in European hospitals. Clin Microbiol Infect 2015; 21(12): 1047–51. doi: 10.1016/j.cmi.2015.09.019 |
| 14. | Voniatis C, Bánsághi S, Ferencz A, Haidegger T. A large-scale investigation of alcohol-based handrub (ABHR) volume: hand coverage correlations utilizing an innovative quantitative evaluation system. Antimicrob Resist Infect Contr 2021; 10(1): 49. 10.1186/s13756-021-00917-8 |
| 15. | Brouqui P, Aladro AS. Alcohol hand rub consumption objectives in European hospitals need to be revisited. Clin Microbiol Infect 2016; 22(6): 577. doi: 10.1016/j.cmi.2016.02.009 |